
Cardiology — MCQs

On this page
Which of the following procedures is contraindicated in Wolff-Parkinson-White syndrome?
A 34-year-old man presents with dyspnea and increasing peripheral edema, following a "flu-like" illness with intermittent sharp left-sided chest pain. On examination, his jugular venous pressure is elevated at 8 cm, heart sounds are soft, and the blood pressure is 104/76 mm Hg, with a 20 mm Hg decrease in systolic arterial pressure during slow inspiration. Which of the following is the most likely diagnosis?
Which of the following is a characteristic EKG finding of ventricular premature beats?
In non-rheumatic atrial fibrillation, which of the following statements is true?
Which of the following statements is false regarding restrictive cardiomyopathy?
What is the characteristic feature of pain experienced in intermittent claudication?
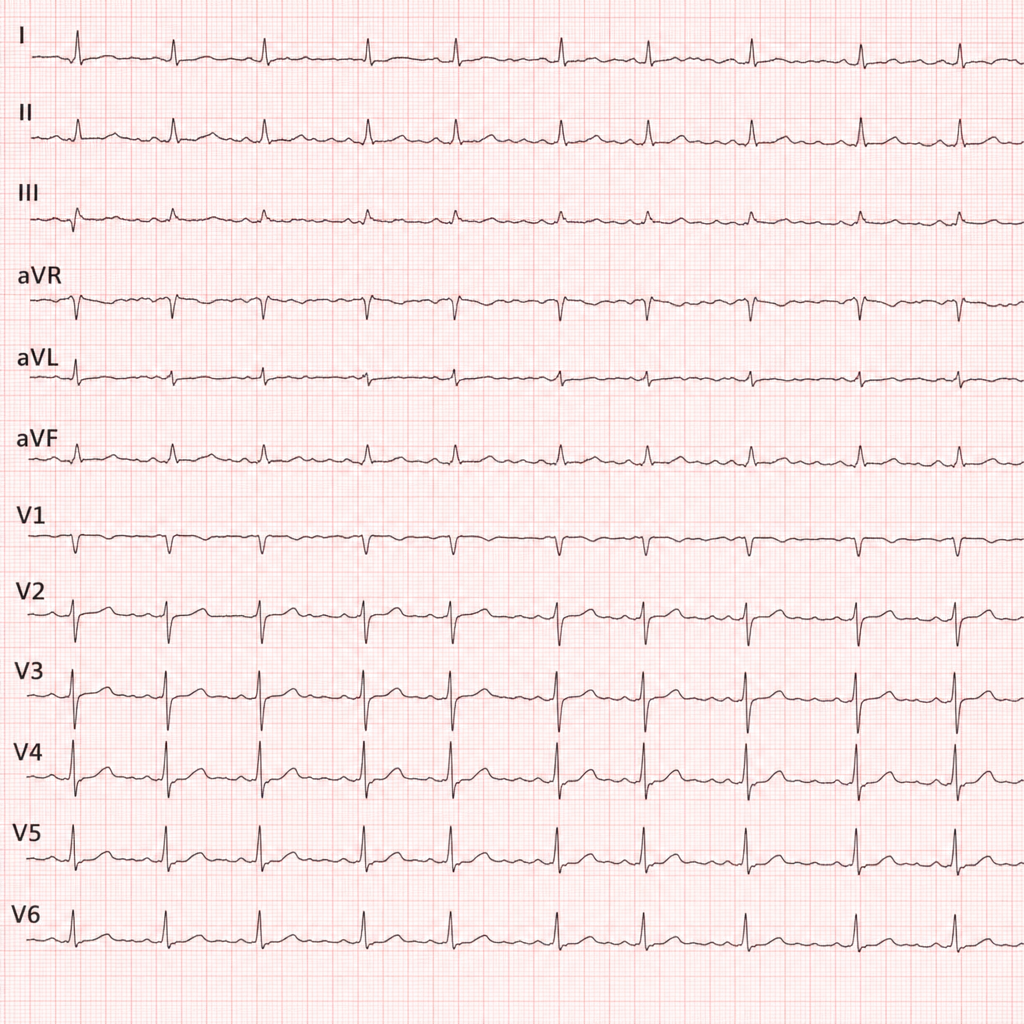
In the ECG shown below, which drug should be avoided in the management of atrial fibrillation?
Which of the following statements is true about infective endocarditis in IV drug abusers?
Which of the following statements regarding the left parasternal lift are NOT true?
Intracavitary electrocardiography is a diagnostic aid in which of the following conditions?
Practice by Chapter
Coronary Artery Disease and Angina
Practice Questions
Acute Coronary Syndromes
Practice Questions
Heart Failure
Practice Questions
Cardiac Arrhythmias
Practice Questions
Valvular Heart Diseases
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease in Adults
Practice Questions
Hypertension and Hypertensive Emergencies
Practice Questions
Pulmonary Hypertension
Practice Questions
Non-invasive Cardiac Diagnostics
Practice Questions
Preventive Cardiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app