
Cardiology — MCQs

On this page
Which score is calculated during the exercise tolerance test for assessing chronic stable angina?
Ebstein's anomaly is associated with which of the following?
What is the threshold for defining a wide QRS duration?
A 65-year-old woman with a history of atherosclerotic cardiovascular disease (ASCVD) presents with palpitations lasting 4 hours. Her heart rate is 180 beats per minute, blood pressure is 90/60 mmHg, and neck veins are distended. Auscultation reveals a carotid artery bruit, a loud S1, and a narrow split S2. Bilateral basal crepitations are noted on chest examination. Which of the following treatments is contraindicated for this patient?
A case of severe mitral stenosis is associated with all of the following features, EXCEPT:
What is the treatment for acute cardiac tamponade?
A 55-year-old woman with metastatic lung cancer presents with dyspnea and pedal edema. On examination, the jugular venous pressure is 10 cm, with a negative Kussmaul's sign. The heart sounds are diminished, and the lungs have bibasilar crackles. The electrocardiogram shows QRS complexes of variable height. For the patient with shortness of breath and peripheral edema, select the most likely diagnosis.
A 45-year-old woman who underwent a modified radical mastectomy 4 years ago and was treated for multiple bone metastases with cyclophosphamide, doxorubicin, and fluorouracil for 6 months is complaining of exertional dyspnea, swelling of the legs, and periorbital edema in the morning. On examination, she has bilateral rales in the lungs, and her cardiovascular examination reveals a palpable S1, S2, S3, and S4 gallop. Her blood pressure is 149/117 mmHg, pulse rate is 80/min, and respiratory rate is 18/min. What is the most likely cause of her cardiac condition?
A patient with native aortic valve disease presents with right hemiparesis. What is the most appropriate management to prevent further stroke?
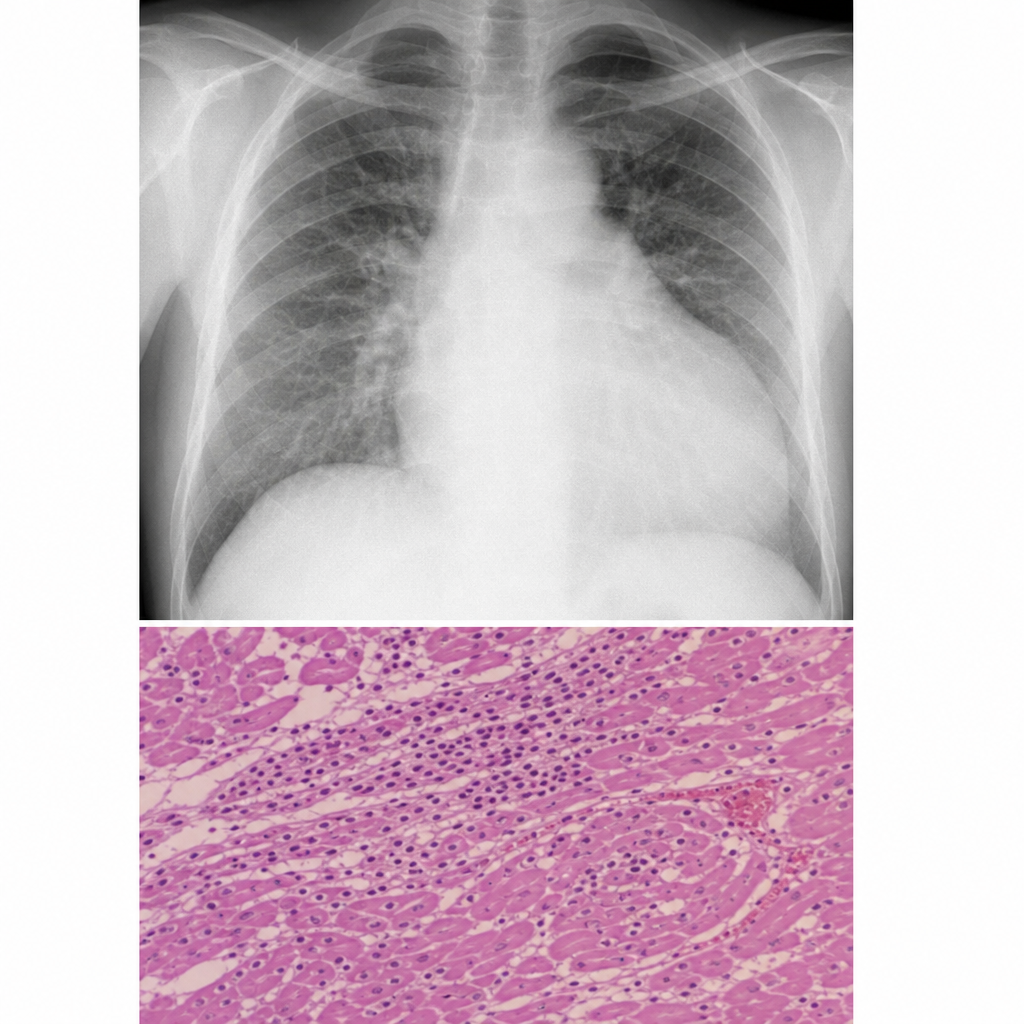
A patient with low cardiac output is having a murmur of mitral regurgitation, and the CXR and histopathology of endomyocardial biopsy are shown. Which type of pulse would be present in this case?
Practice by Chapter
Coronary Artery Disease and Angina
Practice Questions
Acute Coronary Syndromes
Practice Questions
Heart Failure
Practice Questions
Cardiac Arrhythmias
Practice Questions
Valvular Heart Diseases
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease in Adults
Practice Questions
Hypertension and Hypertensive Emergencies
Practice Questions
Pulmonary Hypertension
Practice Questions
Non-invasive Cardiac Diagnostics
Practice Questions
Preventive Cardiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app