
Cardiology — MCQs

On this page
In a patient with subclavian steal syndrome, what is the most characteristic finding?
Extent of cardiotoxicity of chemotherapy and radiotherapy is best diagnosed by:
Which of the following rhythms associated with cardiac arrest is considered shockable?
Reversed Coarctation is seen in which of the following conditions?
Which of the following is true about torsades de pointes?
Ankle-brachial index is useful in prediction of:
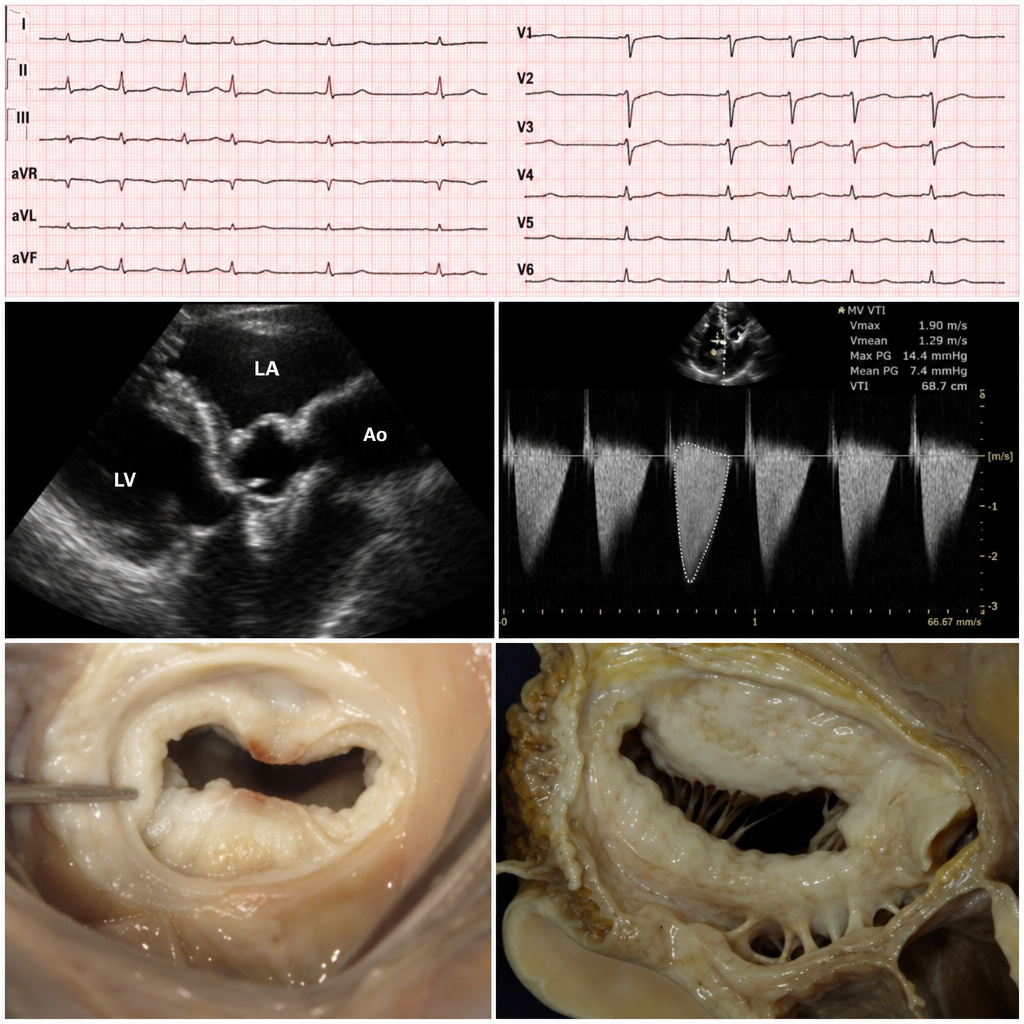
A 28-year-old female presents with progressive dyspnea on exertion and palpitations for the past 6 months. She has a history of recurrent sore throat episodes during childhood. On examination, she has an irregularly irregular pulse, and auscultation reveals a mid-diastolic rumbling murmur at the apex. ECG shows atrial fibrillation with controlled ventricular rate and left atrial enlargement. Echocardiogram demonstrates mitral valve stenosis with commissural fusion, leaflet thickening, and a mitral valve area of 1.2 cm². What is the most likely diagnosis?
Which of the following statements is true regarding the rheumatization of the mitral valve?
Which of the following conditions can lead to an abnormal increase in the amplitude of the 'U' wave on an ECG?
Recommended interventions to reduce the incidence of coronary artery disease include the following except which of the following?
Practice by Chapter
Coronary Artery Disease and Angina
Practice Questions
Acute Coronary Syndromes
Practice Questions
Heart Failure
Practice Questions
Cardiac Arrhythmias
Practice Questions
Valvular Heart Diseases
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease in Adults
Practice Questions
Hypertension and Hypertensive Emergencies
Practice Questions
Pulmonary Hypertension
Practice Questions
Non-invasive Cardiac Diagnostics
Practice Questions
Preventive Cardiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app