
Cardiology — MCQs

On this page
Which of the following is NOT a cause of restrictive cardiomyopathy (RCM)?
Which of the following is not a symptom of carotid atherosclerosis?
What is the recommended management approach for uncomplicated essential hypertension?
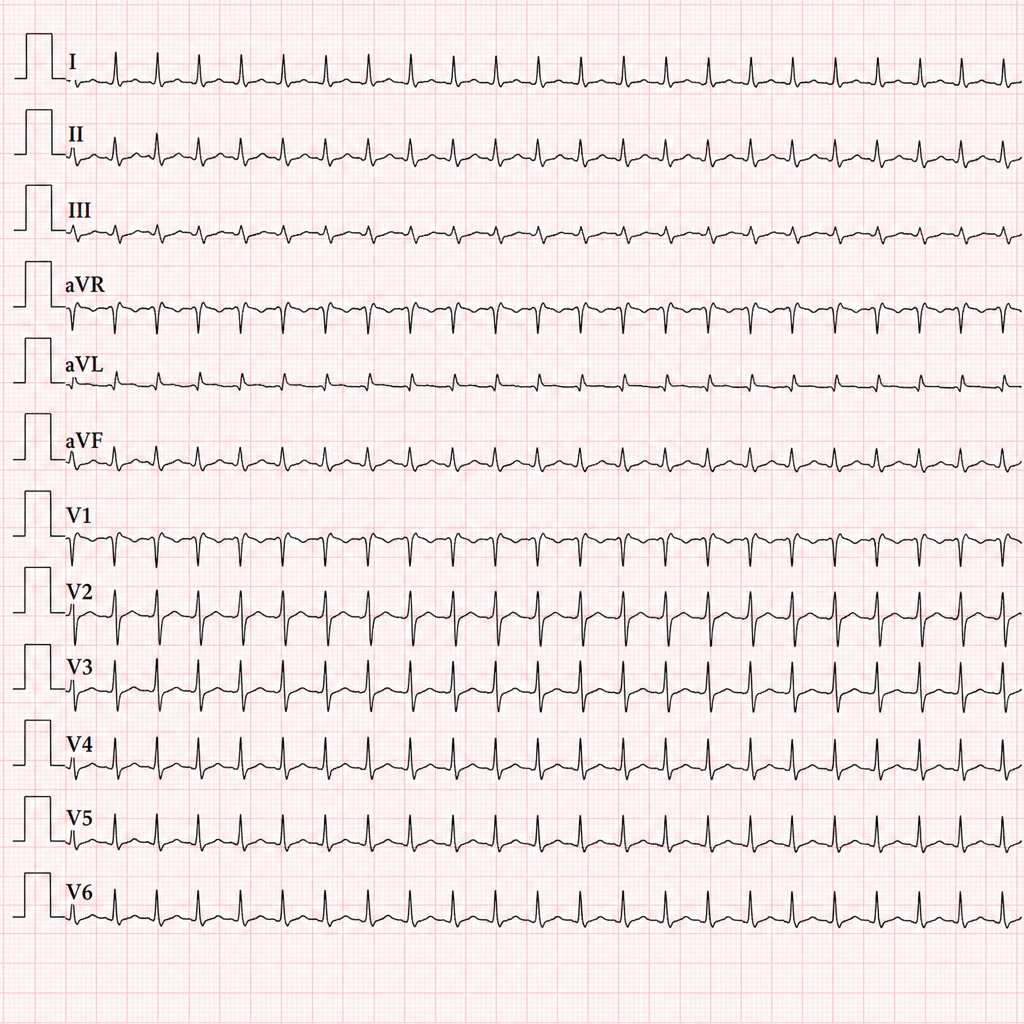
A 22-year-old woman is evaluated in the emergency department because of symptoms of prolonged palpitations. She complains of no associated chest discomfort, shortness of breath, or lightheadedness. The palpitations have occurred twice before, but they always stopped spontaneously after 5 minutes, and she cannot associate them with any triggers. The past health history is negative and she is not on any medications. On physical examination, the blood pressure is 110/70 mm Hg, heart rate is 160/min and regular. The heart and lung examinations are normal, and the ECG is shown in Figure below. After applying carotid sinus pressure, the tachycardia terminates abruptly and sinus rhythm is restored at a heart rate of 72/min. Which of the following is the most likely diagnosis?
Orthostatic hypotension is said to be present if the systolic blood pressure falls by how much while assuming a standing posture from a sitting posture.
Abdominojugular reflex appears after compressing the abdomen for how long?
Which of the following statements about physiological murmurs is false?
A systolic thrill in the left 2nd or 3rd intercostal space is heard in which of the following conditions?
All of the following may cause ST segment elevation on an EKG, except which of the following?
Which of the following is true about the bicuspid aortic valve?
Practice by Chapter
Coronary Artery Disease and Angina
Practice Questions
Acute Coronary Syndromes
Practice Questions
Heart Failure
Practice Questions
Cardiac Arrhythmias
Practice Questions
Valvular Heart Diseases
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease in Adults
Practice Questions
Hypertension and Hypertensive Emergencies
Practice Questions
Pulmonary Hypertension
Practice Questions
Non-invasive Cardiac Diagnostics
Practice Questions
Preventive Cardiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app