
Cardiology — MCQs

On this page
A healthy middle-aged man who became emotionally upset during an argument with his brother suddenly developed chest pain and collapsed. He was declared dead upon arrival at the hospital. What is the most likely diagnosis?
In which condition are epsilon waves observed on an ECG?
Which of the following is the most appropriate true statement regarding ostium primum atrial septal defect (ASD)?
Which is not a major criterion of Jones in rheumatic fever?
A lady presents with grade 3 dyspnea, severe mitral stenosis, and atrial fibrillation, with an increased ventricular rate and a clot in the left atrium. Which of the following should not be done?
What is the best initial pharmacotherapy management option for a 30-year-old male who presents to the emergency department with palpitations, has a regular broad complex tachycardia on ECG, and is haemodynamically stable if DC cardioversion is not available?
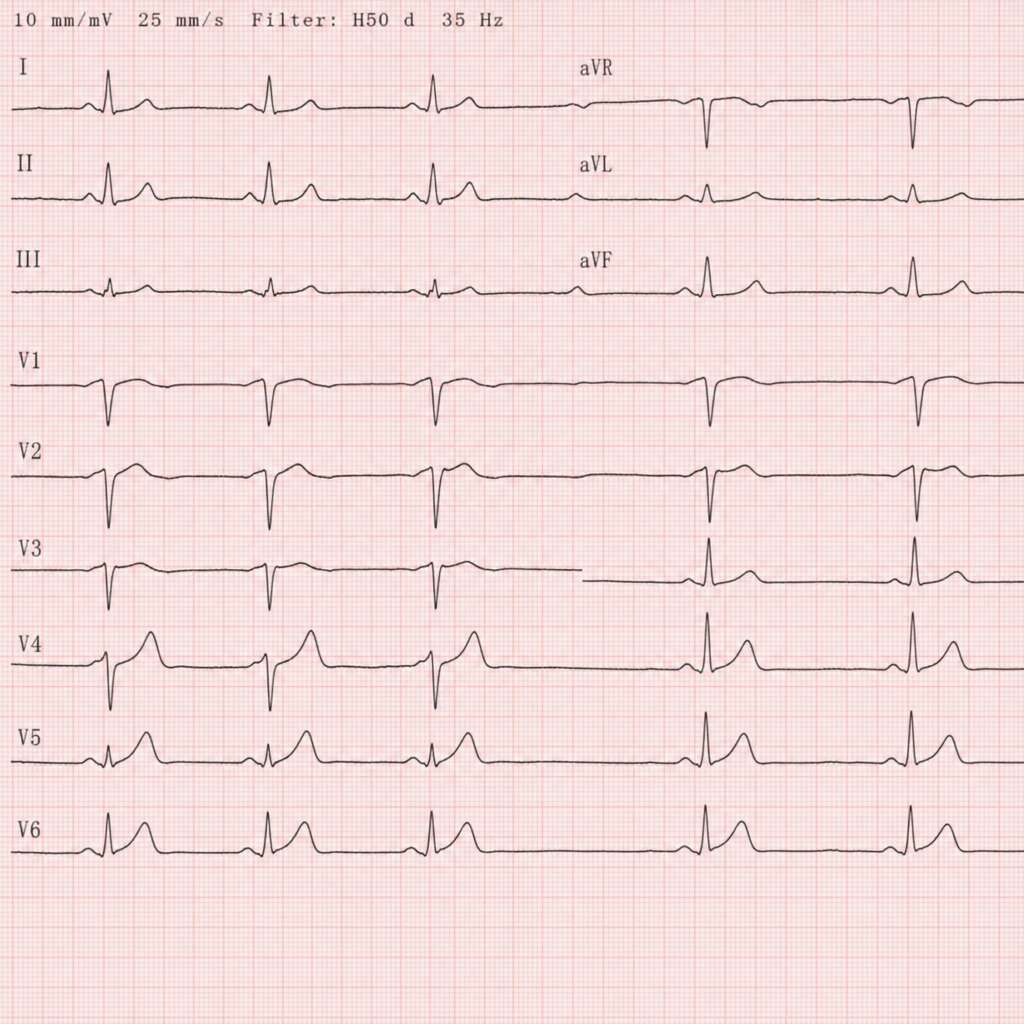
An old lady was brought to the emergency room in an unconscious state, with a history of previous similar attacks in the past months. An ECG was performed, and the resulting graph is shown below. Which of the following arrhythmias is the most probable cause?
What is the best drug for managing atrial flutter with a 4:1 block?
Cardiac biomarker used for diagnosing reinfarction 8 days after initial ischemia is?
Which of the following is a characteristic feature of Takayasu arteritis?
Practice by Chapter
Coronary Artery Disease and Angina
Practice Questions
Acute Coronary Syndromes
Practice Questions
Heart Failure
Practice Questions
Cardiac Arrhythmias
Practice Questions
Valvular Heart Diseases
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease in Adults
Practice Questions
Hypertension and Hypertensive Emergencies
Practice Questions
Pulmonary Hypertension
Practice Questions
Non-invasive Cardiac Diagnostics
Practice Questions
Preventive Cardiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app