
Cardiology — MCQs

On this page
A 69-year-old man complains of chest tightness and shortness of breath after lifting boxes 3 hours ago. He perceives that his heart is skipping beats. His medical history is significant for hypertension and cigarette smoking. On examination, his heart rate is 50 beats/min and regular, and his lungs are clear to auscultation. An electrocardiogram shows bradycardia with an increased PR interval and ST-segment elevation in multiple leads including the anterior leads, V1 and V2. What anatomical structures are most likely affected?
The murmur of hypertrophic obstructive cardiomyopathy is decreased in which of the following positions or maneuvers?
Which of the following is true about the pain of pericarditis?
What is the most common cause of native valve endocarditis?
What are the ECG changes of hypomagnesemia?
A 72-year-old male presents with intermittent symptoms of dyspnea on exertion, palpitations, and occasional blood-streaked cough. Cardiac auscultation reveals a faint, low-pitched diastolic rumbling murmur heard best at the apex. What is the most probable underlying cause of the patient's symptoms?
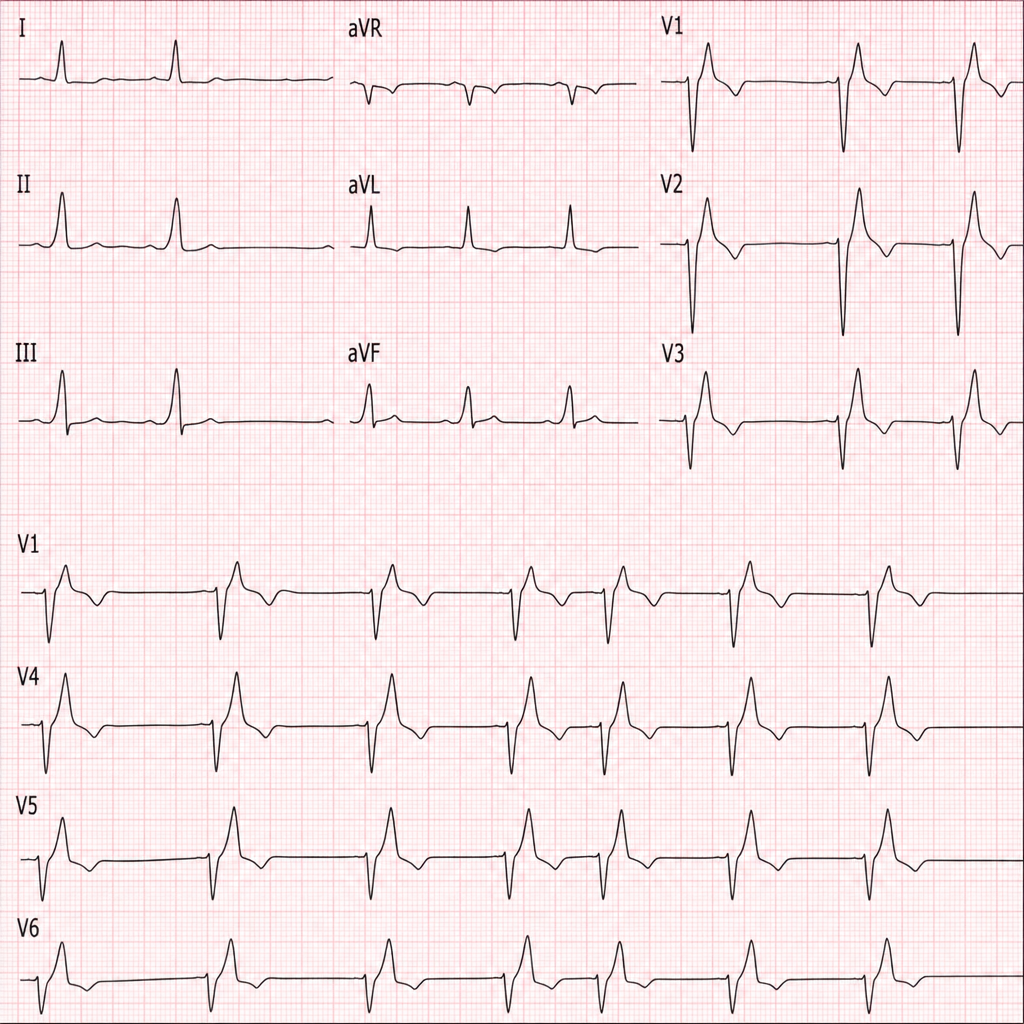
Which of the following conditions is most likely to cause these ECG changes?
Which of the following can NOT be used to treat peripheral arterial disease?
Prophylactic antibiotic coverage before dental extraction is indicated for all the following conditions except:
Reciprocal ST depression in leads V1-V3 is typically seen in which type of myocardial infarction?
Practice by Chapter
Coronary Artery Disease and Angina
Practice Questions
Acute Coronary Syndromes
Practice Questions
Heart Failure
Practice Questions
Cardiac Arrhythmias
Practice Questions
Valvular Heart Diseases
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease in Adults
Practice Questions
Hypertension and Hypertensive Emergencies
Practice Questions
Pulmonary Hypertension
Practice Questions
Non-invasive Cardiac Diagnostics
Practice Questions
Preventive Cardiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app