
Cardiology — MCQs

On this page
Hockey stick appearance on echo is a feature of.
Positive hepatojugular reflux is found in all of the following conditions except -
Which of the following statements regarding hypertensive crisis is false?
What is an electrical storm?
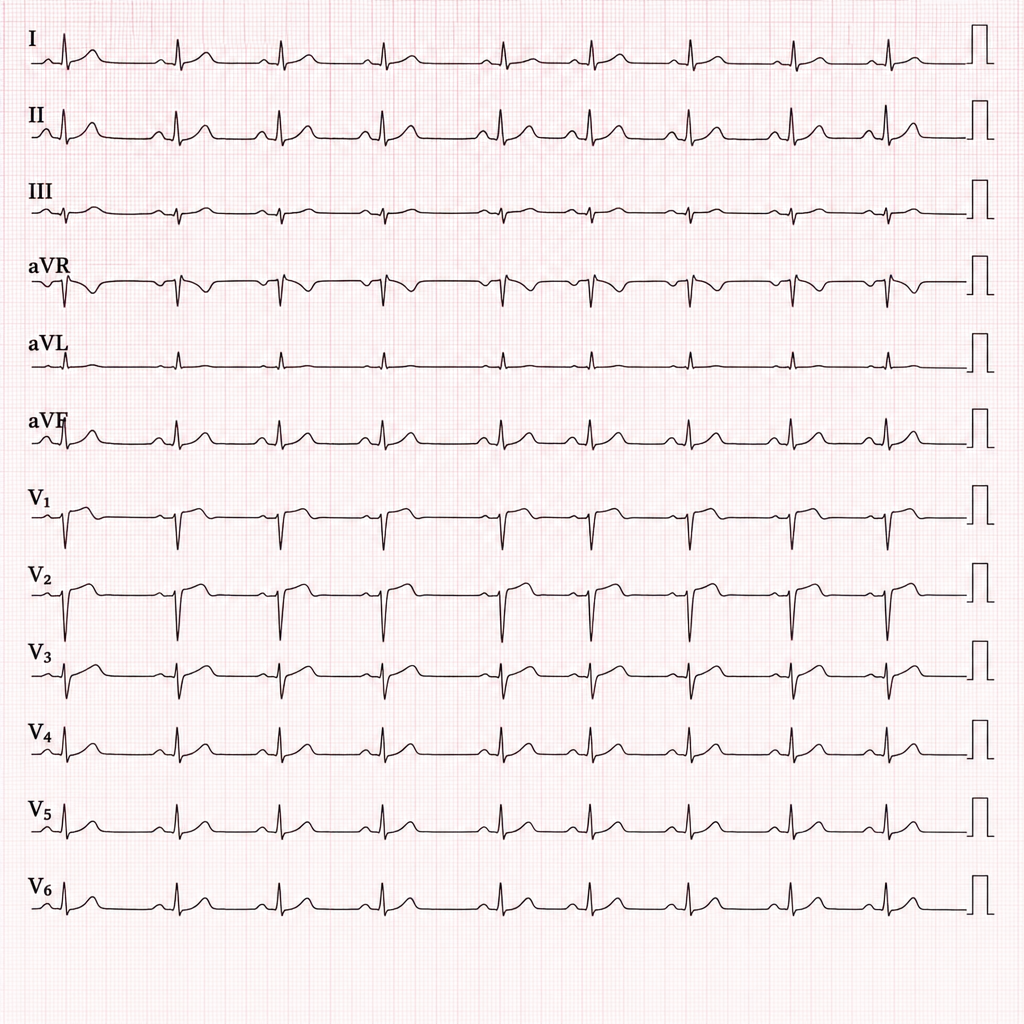
A 45-year-old man presents to the emergency department with sudden onset shortness of breath and pleuritic chest pain. He recently returned from a long-haul flight. His heart rate is 112 bpm and oxygen saturation is 91% on room air. The given ECG shows the following findings:
What is the immediate treatment modality for a patient presenting with acute anterior wall myocardial infarction and hypotension?
Accelerated idioventricular rhythm (AIVR) is most characteristically seen in?
What is the most common site of acute aortic dissection?
Duration of pain in angina is:
In acute left ventricular failure with pulmonary edema, which drug can be administered for immediate management?
Practice by Chapter
Coronary Artery Disease and Angina
Practice Questions
Acute Coronary Syndromes
Practice Questions
Heart Failure
Practice Questions
Cardiac Arrhythmias
Practice Questions
Valvular Heart Diseases
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease in Adults
Practice Questions
Hypertension and Hypertensive Emergencies
Practice Questions
Pulmonary Hypertension
Practice Questions
Non-invasive Cardiac Diagnostics
Practice Questions
Preventive Cardiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app