
Cardiology — MCQs

On this page
In a patient with heart disease, which condition is most commonly associated with left atrial enlargement?
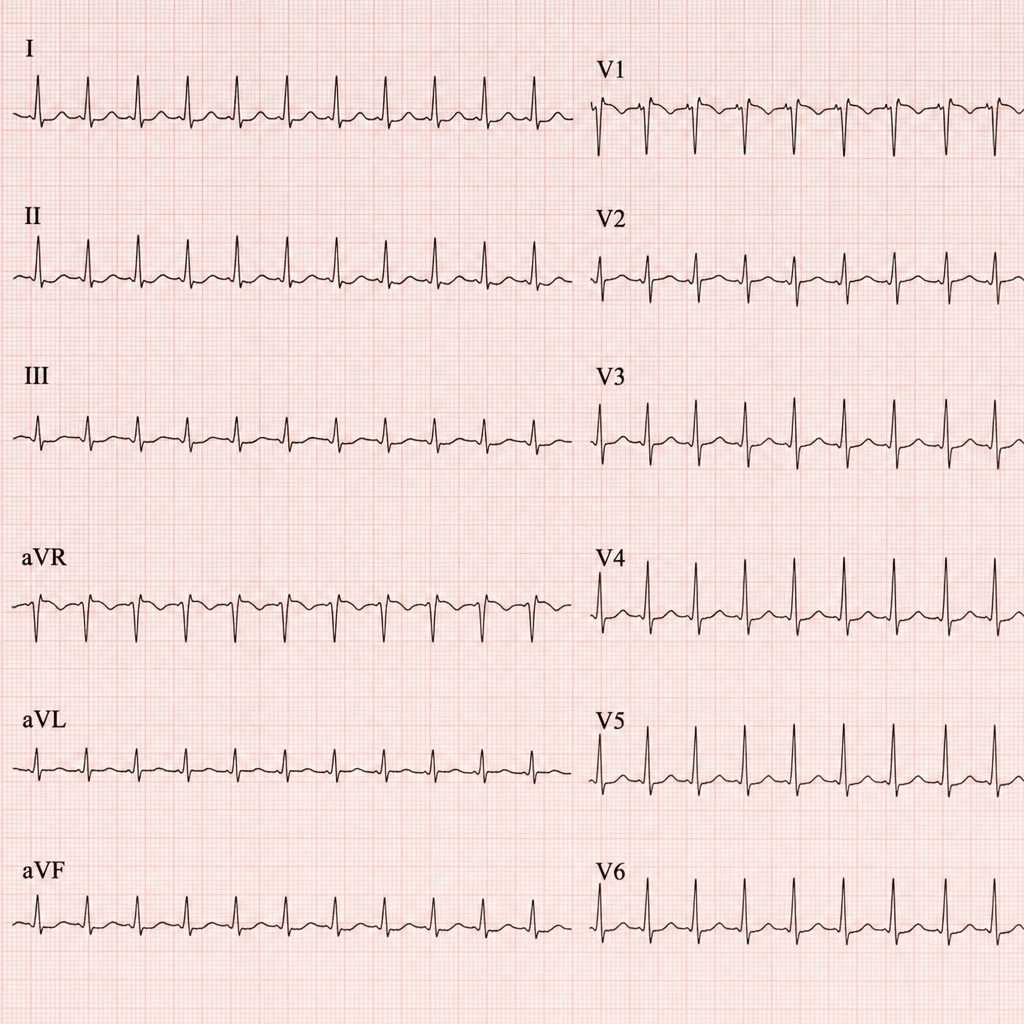
Refer to the provided ECG image. It demonstrates which of the following?
In which of the following conditions is differential cyanosis observed?
Torsades de pointes is seen in all except
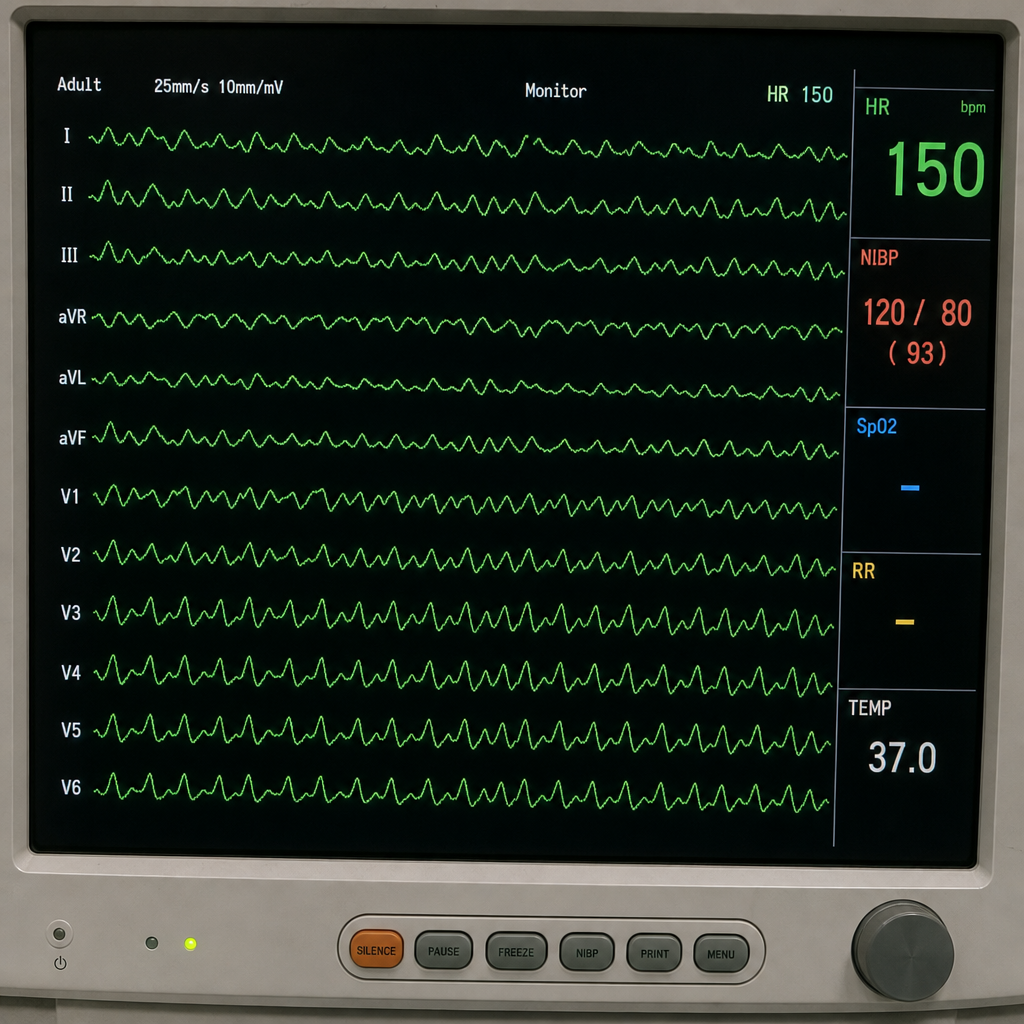
This patient came to the casualty with palpitations. His ECG has been shown below. What is your diagnosis?
Subclavian steal syndrome is
What is the most likely cause of fluid overload in a patient presenting with shortness of breath?
Graham Steell murmur is associated with which of the following conditions?
Which of the following is associated with WPW syndrome?
Under which condition are steroids administered in rheumatic fever?
Practice by Chapter
Coronary Artery Disease and Angina
Practice Questions
Acute Coronary Syndromes
Practice Questions
Heart Failure
Practice Questions
Cardiac Arrhythmias
Practice Questions
Valvular Heart Diseases
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease in Adults
Practice Questions
Hypertension and Hypertensive Emergencies
Practice Questions
Pulmonary Hypertension
Practice Questions
Non-invasive Cardiac Diagnostics
Practice Questions
Preventive Cardiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app