
Cardiology — MCQs

On this page
What is the most appropriate immediate management for a hemodynamically unstable patient with supraventricular tachycardia (SVT)?
Which of the following statements is true about the Bundle of Kent?
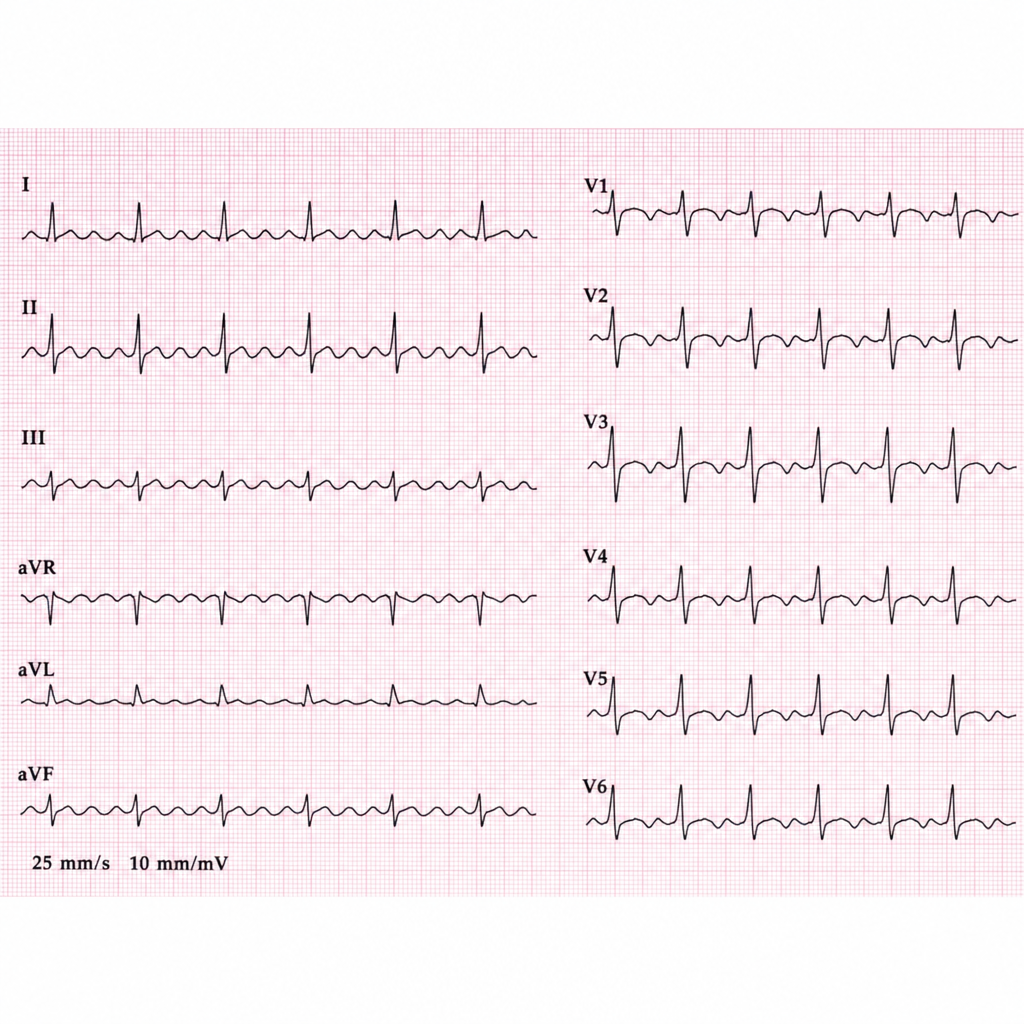
Identify the condition in the provided ECG image.
A patient presents to you with an irregularly irregular pulse of 120/minutes and a pulse deficit of 20. Which of the following would be the jugular venous pressure (JVP) finding?
Osborn J waves are seen in which of the following conditions?
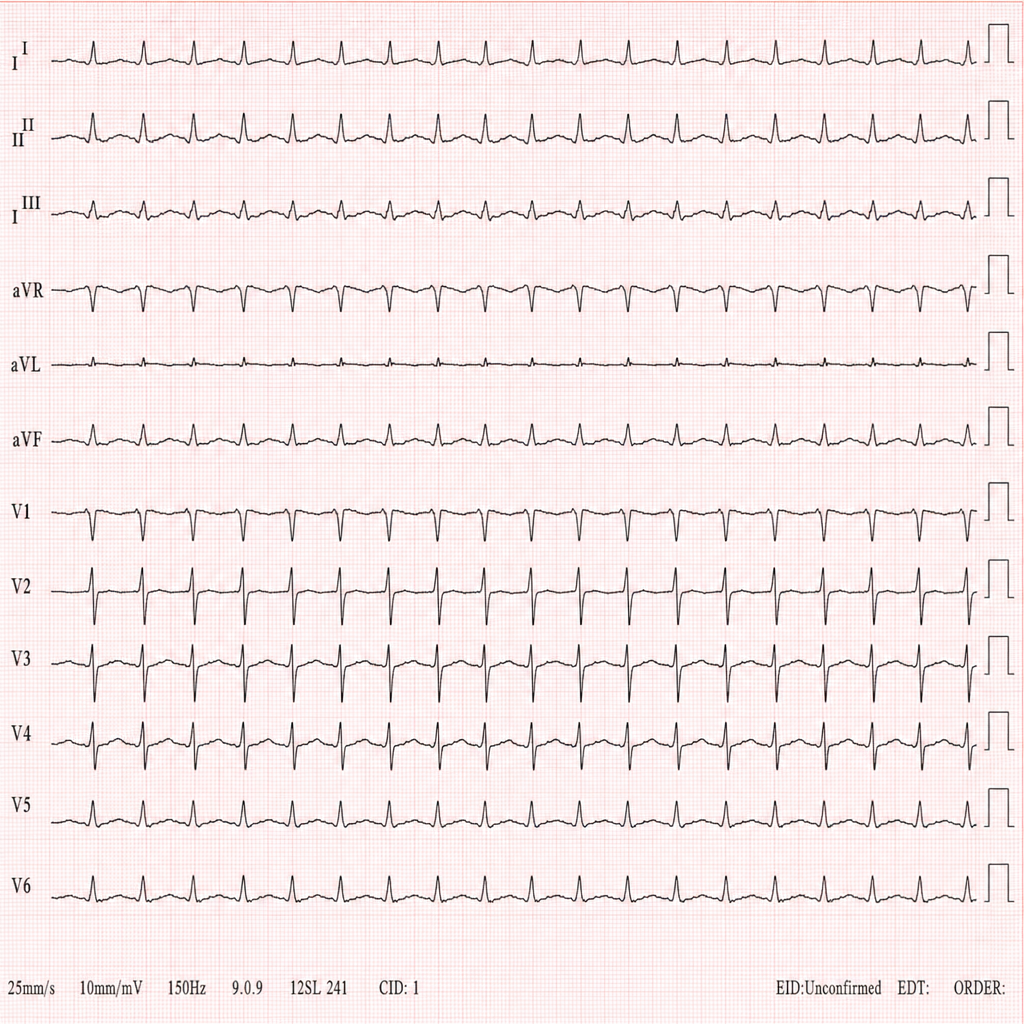
A 32-year-old patient presents to the emergency department with palpitations and dizziness. He reports that the episode started abruptly. An ECG is obtained showing a regular narrow-complex tachycardia at 180 bpm with pseudo-R′ waves visible in lead V1, consistent with retrograde P-waves. When adenosine is administered, the tachycardia terminates abruptly. Identify the cardiac rhythm shown in the image.
What are the potential causes of cardiogenic shock excluding myocardial infarction?
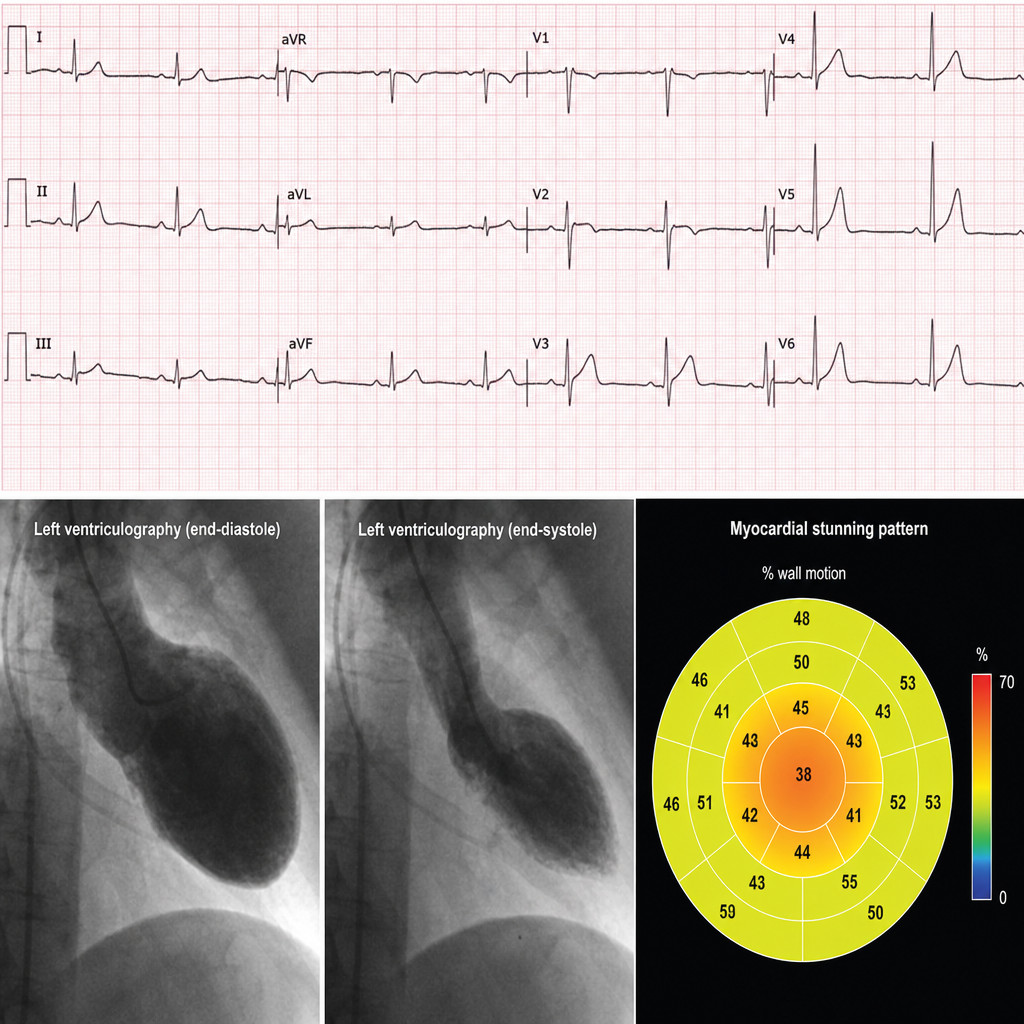
In a patient presenting with an ECG that shows ST-segment elevation but with a myocardial stunning pattern that does not correspond to a single coronary artery territory, what is the most likely diagnosis?
In which of the following conditions is the implantation of an Automatic Implantable Cardioverter Defibrillator (AICD) indicated?
Roth spots are associated with which of the following conditions?
Practice by Chapter
Coronary Artery Disease and Angina
Practice Questions
Acute Coronary Syndromes
Practice Questions
Heart Failure
Practice Questions
Cardiac Arrhythmias
Practice Questions
Valvular Heart Diseases
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease in Adults
Practice Questions
Hypertension and Hypertensive Emergencies
Practice Questions
Pulmonary Hypertension
Practice Questions
Non-invasive Cardiac Diagnostics
Practice Questions
Preventive Cardiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app