
Cardiology — MCQs

On this page
Treatment of asymptomatic bradycardia is
The normal range for Ankle Brachial Pressure Index (ABI) is:
LBBB is seen with all except
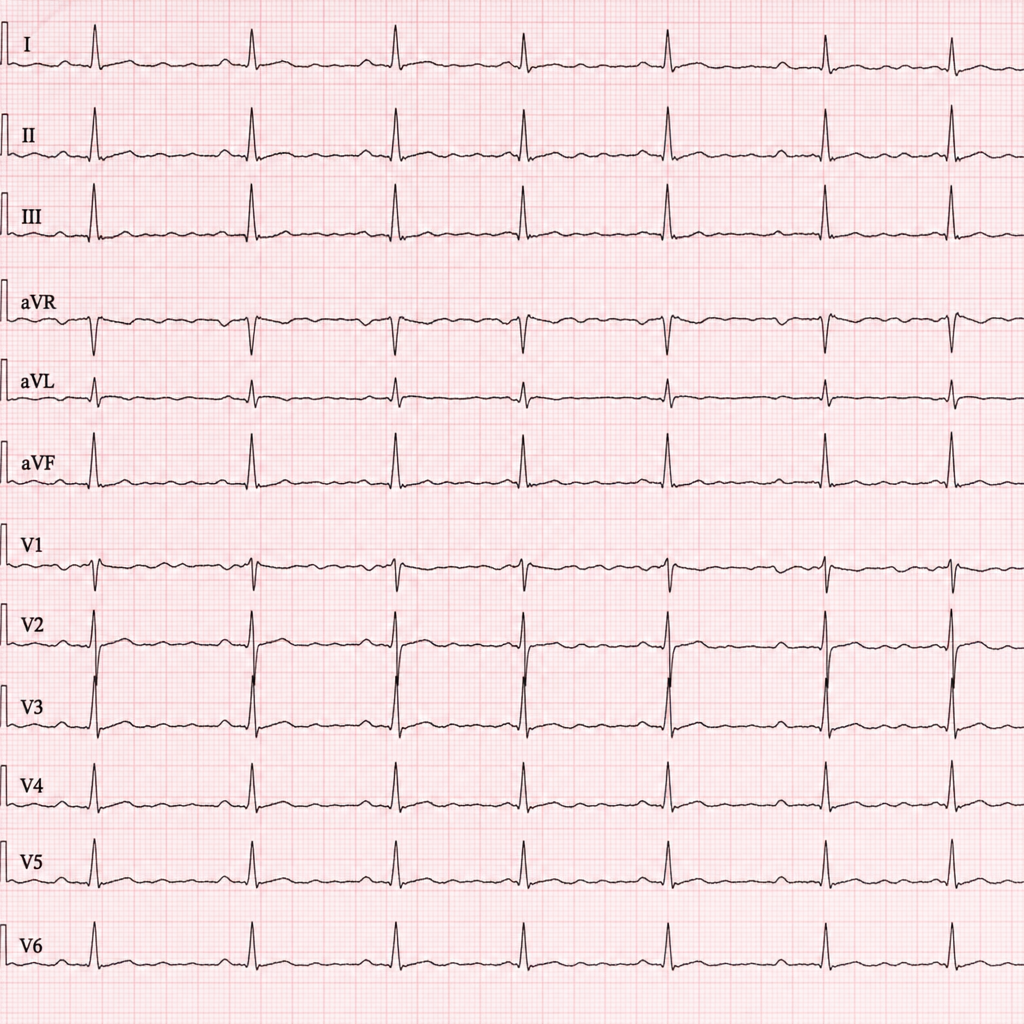
A patient in regular rhythm presents with absent P waves on ECG. Which of the following is the most likely diagnosis based on the ECG findings?
The S2 heart sound is best appreciated in:
Erb's Point in cardiology refers to:
Which of the following is the MOST common complication of untreated hypertension?
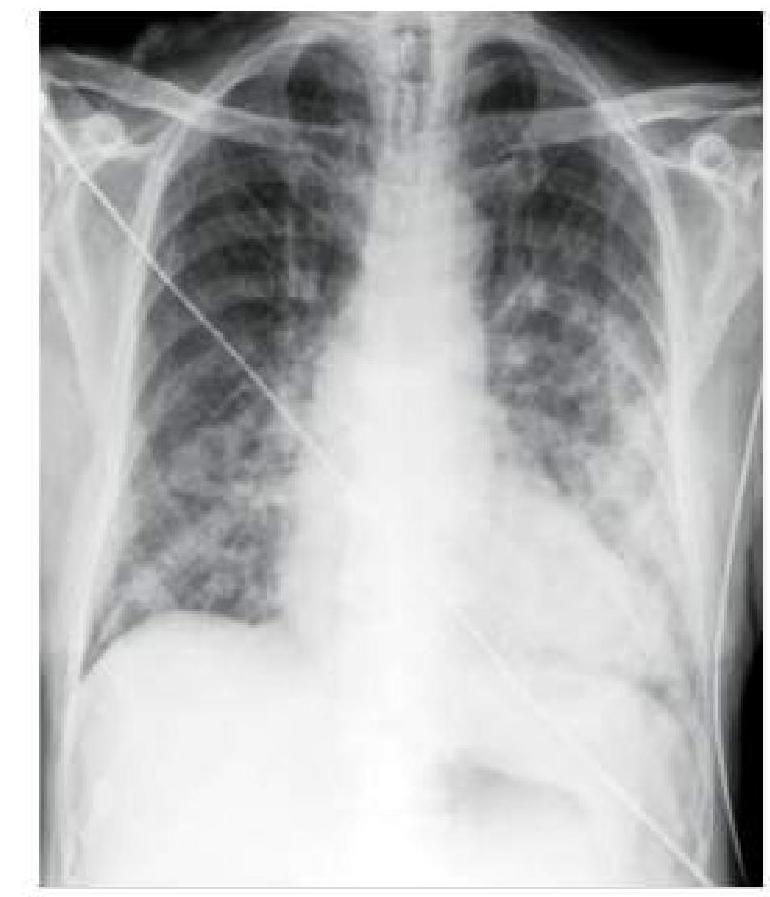
A hypertensive patient who is non-compliant with medication presents to you with sudden onset breathlessness. His blood pressure is 190/110 mmHg and oxygen saturation is 88% on room air. A chest x-ray was done, which is shown below. How will you manage this patient?
Which type of cardiomyopathy is associated with alcohol abuse?
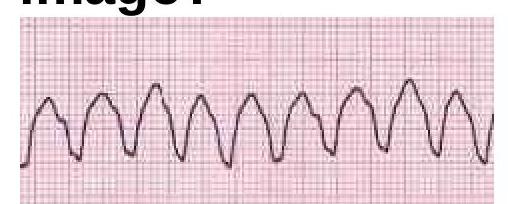
Identify the cardiac condition represented in the image.
Practice by Chapter
Coronary Artery Disease and Angina
Practice Questions
Acute Coronary Syndromes
Practice Questions
Heart Failure
Practice Questions
Cardiac Arrhythmias
Practice Questions
Valvular Heart Diseases
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease in Adults
Practice Questions
Hypertension and Hypertensive Emergencies
Practice Questions
Pulmonary Hypertension
Practice Questions
Non-invasive Cardiac Diagnostics
Practice Questions
Preventive Cardiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app