
Cardiology — MCQs

On this page
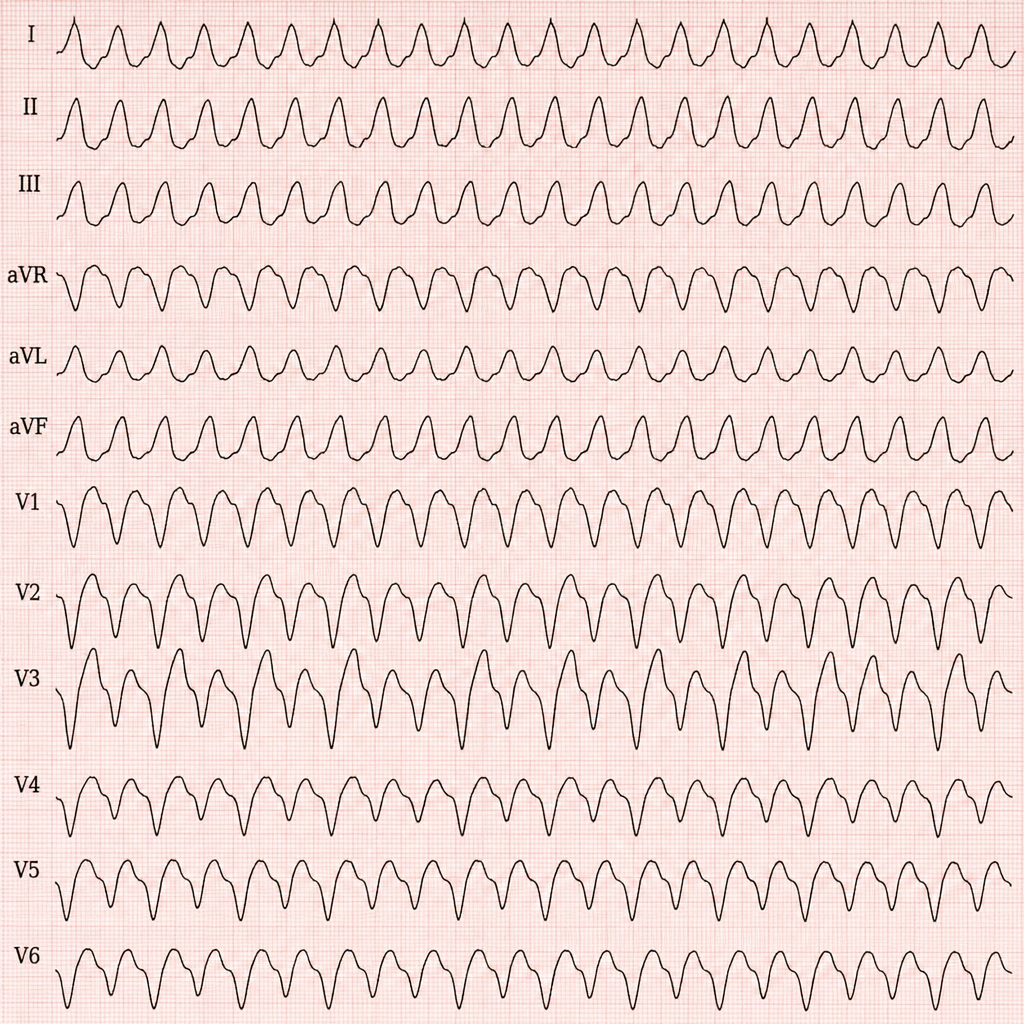
A patient presents with a regular wide QRS complex tachycardia (QRS >0.12 seconds) at a rate of 160 bpm. The ECG shows AV dissociation with fusion beats and capture beats. What is the most likely cardiac condition?
Which murmur increases on standing?
Identify the condition in the ECG based on the provided image.
What is the immediate treatment for a hemodynamically unstable patient with supraventricular tachycardia (SVT)?

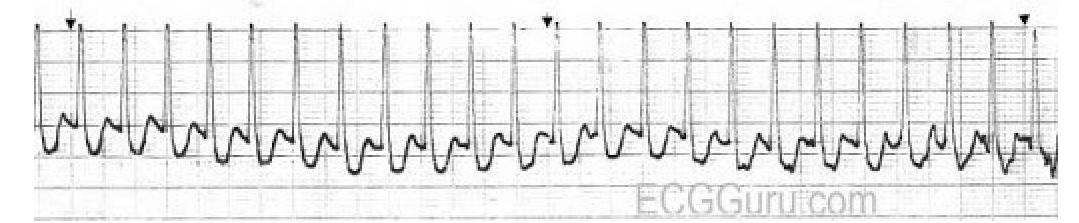
Which rhythm classification is best supported by this single-lead ECG tracing?
A patient presents with chest pain and an ECG showing ST-segment elevation. After treatment, the ECG shows resolution of ST-segment changes, but the patient continues to have chest pain. What is the most likely diagnosis?
What is a potential cause of cardiogenic shock other than myocardial infarction (MI)?
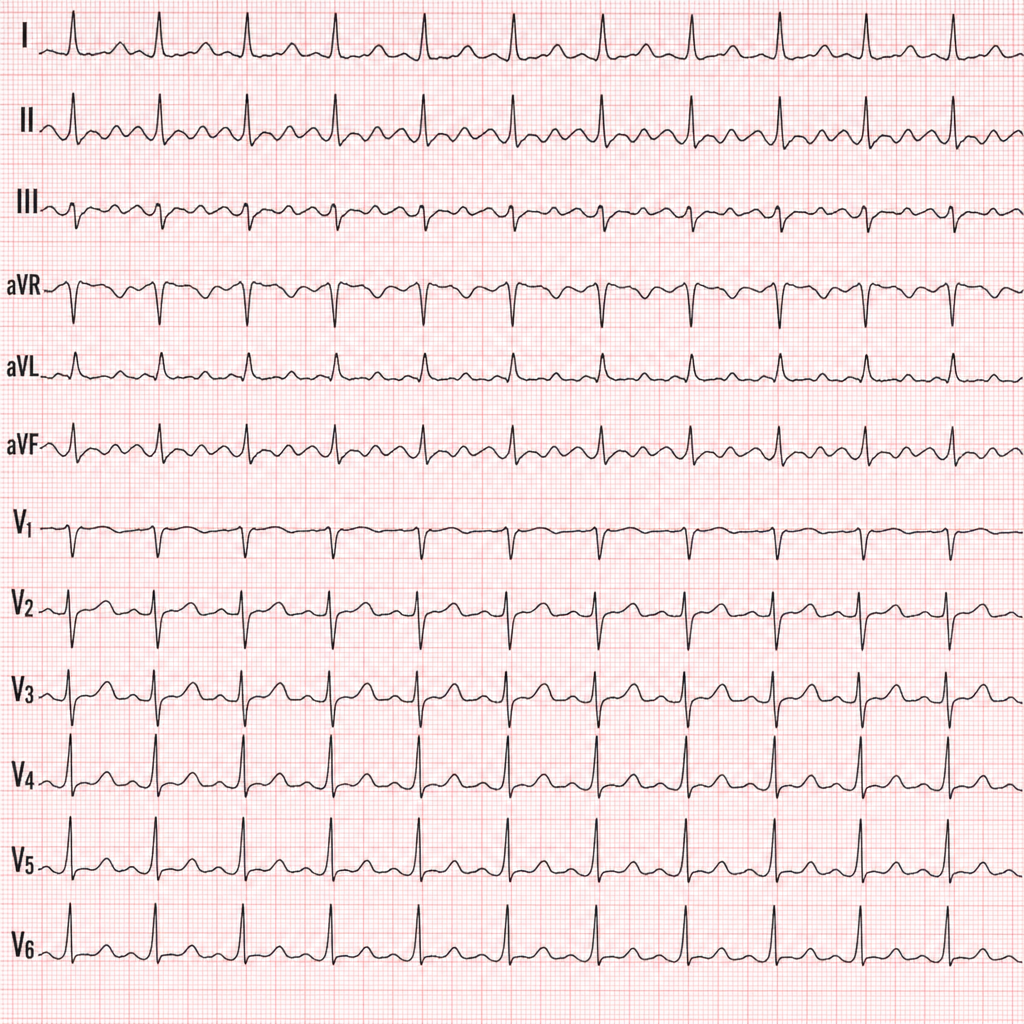
Which condition is associated with the ECG pattern known as pseudo P pulmonale?
At what time frame does peripartum cardiomyopathy typically occur?
Downhill esophageal varices develop as a result of obstruction of which vein?
Practice by Chapter
Coronary Artery Disease and Angina
Practice Questions
Acute Coronary Syndromes
Practice Questions
Heart Failure
Practice Questions
Cardiac Arrhythmias
Practice Questions
Valvular Heart Diseases
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease in Adults
Practice Questions
Hypertension and Hypertensive Emergencies
Practice Questions
Pulmonary Hypertension
Practice Questions
Non-invasive Cardiac Diagnostics
Practice Questions
Preventive Cardiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app