
Cardiology — MCQs

On this page
A patient presents with palpitations, chest pain, and irregular pulse. ECG shows irregular RR intervals with no P waves. Diagnosis?
A 55-year-old diabetic presents with chest pain, shortness of breath, and diaphoresis that began 1 hour ago. He has no history of prior stroke, recent surgery, or other contraindications to fibrinolysis. ECG shows ST elevation. A PCI-capable catheterization laboratory is immediately available and primary PCI can be performed within the guideline-recommended timeframe. What is the next best step?
A 55-year-old diabetic man presents to a PCI-capable hospital with chest pain, shortness of breath, and diaphoresis for the past 2 hours. ECG shows ST elevation. The estimated door-to-balloon time at this facility is 65 minutes. What is the next best step in management?
A 30-year-old female presents with exertional dyspnea and a loud P2 on auscultation. What is the most likely diagnosis?
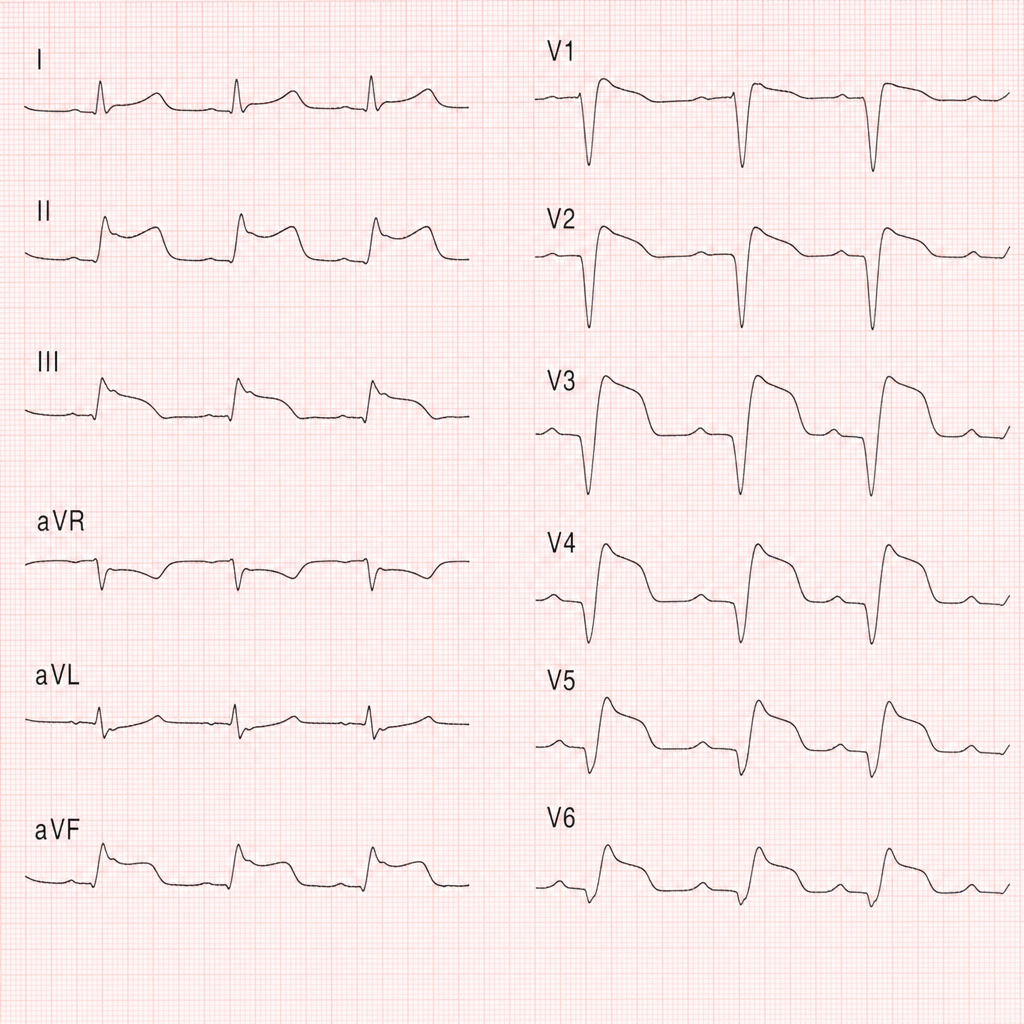
Which condition is indicated by 'Q waves' and 'ST elevation' in leads II, III, and aVF?
Which of the following statements about atrial fibrillation is correct?
A 65-year-old female with a history of heart failure presents with new-onset ascites and peripheral edema. What is the most likely underlying cause of her ascites?
A 65M presents with worsening dyspnea and leg swelling. Physical examination reveals an elevated jugular venous pressure and bilateral lower extremity pitting edema. Most likely cause of his symptoms?
Which of the following is the most common cause of acute dyspnea in elderly adults?
A 65-year-old man with congestive heart failure presents with worsening bilateral pitting edema. What is the most appropriate next step in management?
Practice by Chapter
Coronary Artery Disease and Angina
Practice Questions
Acute Coronary Syndromes
Practice Questions
Heart Failure
Practice Questions
Cardiac Arrhythmias
Practice Questions
Valvular Heart Diseases
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease in Adults
Practice Questions
Hypertension and Hypertensive Emergencies
Practice Questions
Pulmonary Hypertension
Practice Questions
Non-invasive Cardiac Diagnostics
Practice Questions
Preventive Cardiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app