
Cardiology — MCQs

On this page
Which of the following is a major criterion of Rheumatic fever according to Jones criteria? a) Chorea b) Erythema nodosum c) Arthritis d) Fever e) Carditis
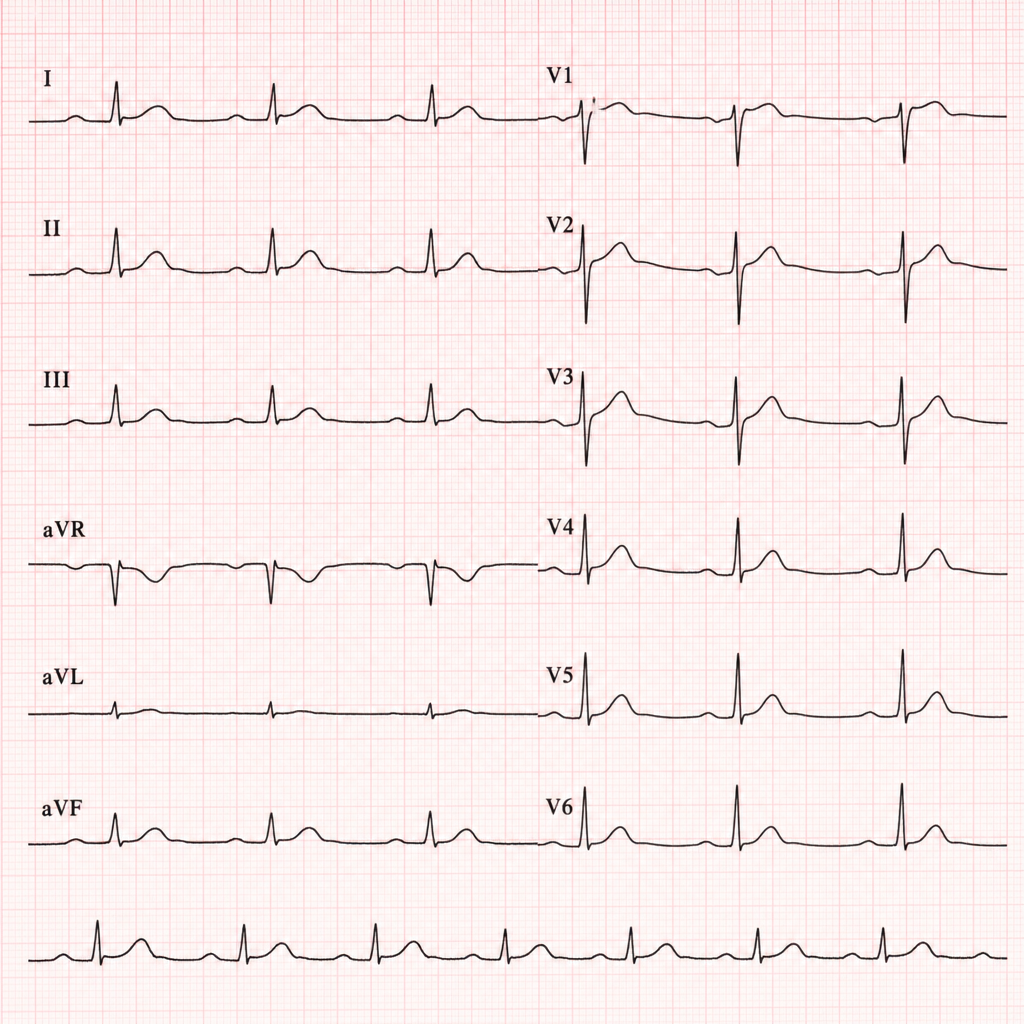
A previously healthy patient presents with dyspnea and low grade fever since 4 months. His lungs are clear. JVP is normal. ECG showed low voltage complexes. What is the possible diagnosis?
Most common cause of death in Rheumatoid Arthritis?
Most common cause of death in adults with PDA is?
Cardiotoxicity caused by radiotherapy & chemotherapy is best detected by
Essential criteria for TOF includes all except ?
A 30 year old male was brought to the ER after a car crash. On admission, pulse is weak with BP=80/60 mmHg. Jugular venous pressure is elevated, heart sounds are muffled, and bedside echocardiography reveals a pericardial effusion with right ventricular diastolic collapse consistent with cardiac tamponade. A right-heart catheter is placed. Which is the most consistent value with patient's diagnosis?
A young female presents with chest pain not associated with exercise. Auscultation reveals multiple ejection clicks with a murmur. The most important investigation for diagnosis is:
Obstruction in pulmonary stenosis may occur at the following sites ___________
Which lipid parameter is most useful for cardiovascular risk stratification in hypertensive patients?
Practice by Chapter
Coronary Artery Disease and Angina
Practice Questions
Acute Coronary Syndromes
Practice Questions
Heart Failure
Practice Questions
Cardiac Arrhythmias
Practice Questions
Valvular Heart Diseases
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease in Adults
Practice Questions
Hypertension and Hypertensive Emergencies
Practice Questions
Pulmonary Hypertension
Practice Questions
Non-invasive Cardiac Diagnostics
Practice Questions
Preventive Cardiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app