
Diseases of the Nose and Paranasal Sinuses — MCQs

On this page
The Caldwell-Luc procedure is performed to access which anatomical space?
All of the following are part of Samter's triad except?
A 4-year-old child presents with bleeding from the right side of the nose. He also has purulent discharge from the same side. What is the most likely diagnosis?
During extraction of an upper first molar, the mesiobuccal root is missing and suspected to have been pushed into the maxillary sinus. To classify a chronic oral-antral communication, what time duration is acceptable?
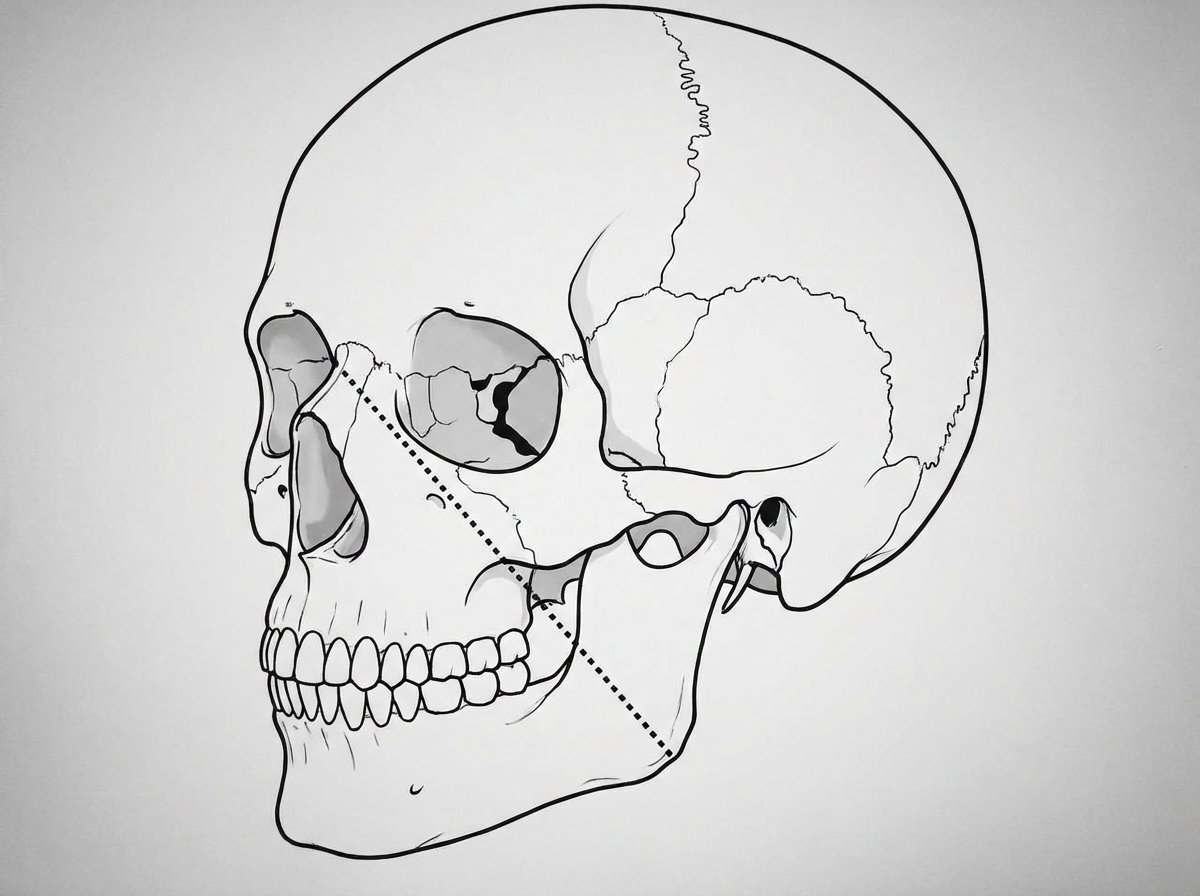
The dotted line has clinical significance in case of which of the following conditions?
A 70-year-old patient presents with a history of epistaxis. On examination, the blood pressure is 200/100 mm Hg. No active nasal bleeding is noted at the time of examination. What is the next step in management?
Improvement in nasal patency by retracting the lateral part of the cheek and thus testing the vestibular component of the nose is called what?
What is true about nasal myiasis?
Lines of Sebileau pass through which structures?
What is the most definitive diagnostic method for sinusitis?
Practice by Chapter
Rhinitis
Practice Questions
Acute Rhinosinusitis
Practice Questions
Chronic Rhinosinusitis
Practice Questions
Nasal Polyposis
Practice Questions
Allergic Fungal Sinusitis
Practice Questions
Deviated Nasal Septum
Practice Questions
Epistaxis
Practice Questions
Nasal Trauma
Practice Questions
Choanal Atresia
Practice Questions
CSF Rhinorrhea
Practice Questions
Tumors of the Nose and Paranasal Sinuses
Practice Questions
Complications of Sinusitis
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app