
Diseases of the Nose and Paranasal Sinuses — MCQs

On this page
A 35-year-old female patient presents with complaints of nasal obstruction and post-nasal drip. There is a past history of FESS for failed conservative management 5 years ago. Uncinectomy and maxillary ostium dilation was done during the previous FESS. A DNE done now shows patent ostia and mucosal edema of the maxillary sinus lining. What is the next best step in management? FESS - Functional endoscopic sinus surgery
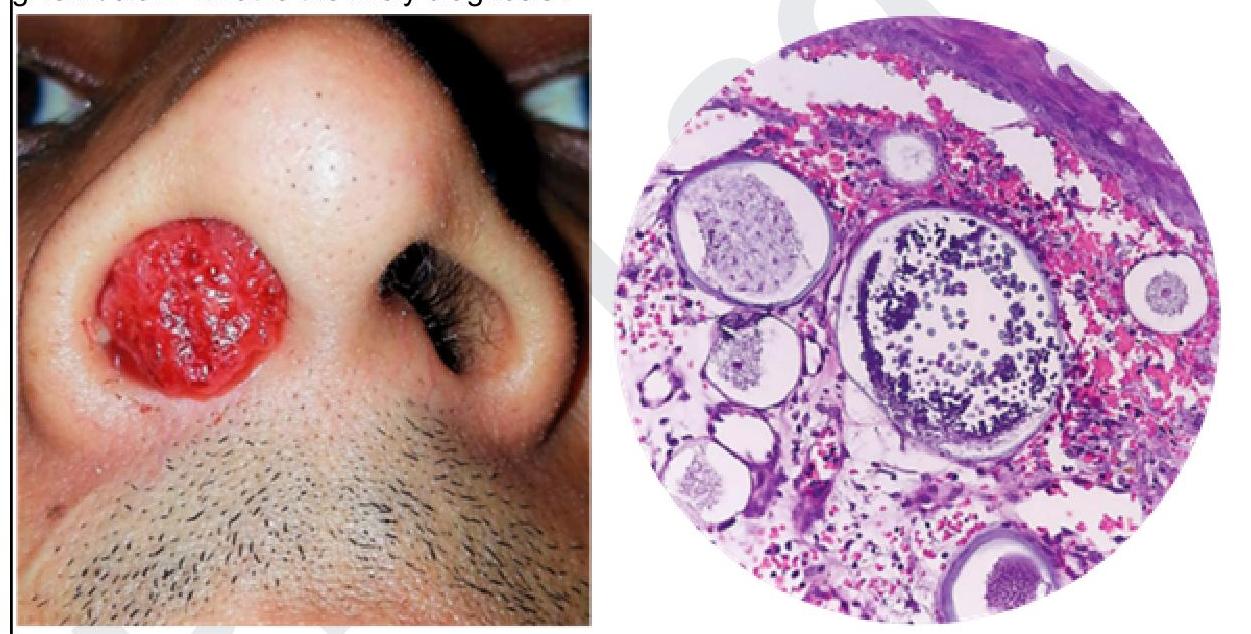
A South Indian male farmer presents to the ENT OPD with complaints of reddish mass coming out from the nose as shown in the image below and the histopathology examination is also given below. What is the likely diagnosis?
Young's operation is done for:
Frontal headache is due to inflammation of which sinus?
Most common malignancy of maxillary antrum:
A young boy came to OPD with complaints of difficulty in breathing. On examination, bilateral polyps were found. On aspiration, bleeding was seen. What will be the initial management?
Most prominent and largest air cell of ethmoidal sinus?
Rhinoscleroma, true statement is:
Failure of rupture of buccopharyngeal membrane leads to?
CSF rhinorrhea is diagnosed by: MP 07
Practice by Chapter
Rhinitis
Practice Questions
Acute Rhinosinusitis
Practice Questions
Chronic Rhinosinusitis
Practice Questions
Nasal Polyposis
Practice Questions
Allergic Fungal Sinusitis
Practice Questions
Deviated Nasal Septum
Practice Questions
Epistaxis
Practice Questions
Nasal Trauma
Practice Questions
Choanal Atresia
Practice Questions
CSF Rhinorrhea
Practice Questions
Tumors of the Nose and Paranasal Sinuses
Practice Questions
Complications of Sinusitis
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app