
Diseases of the Nose and Paranasal Sinuses — MCQs

On this page
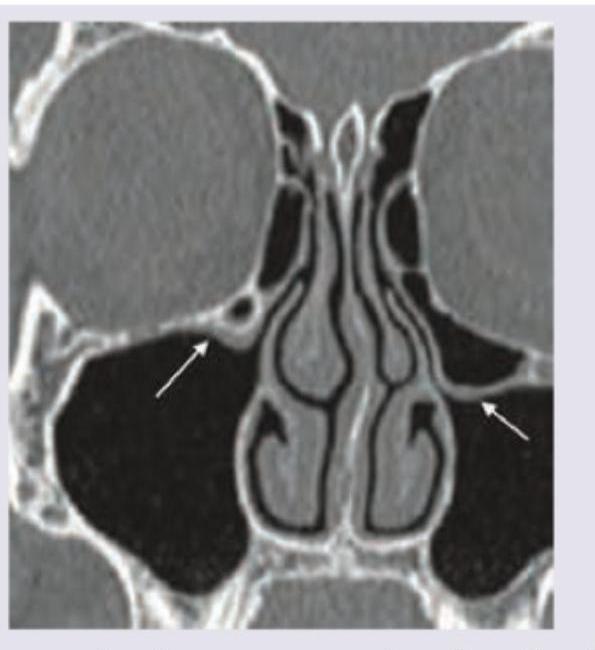
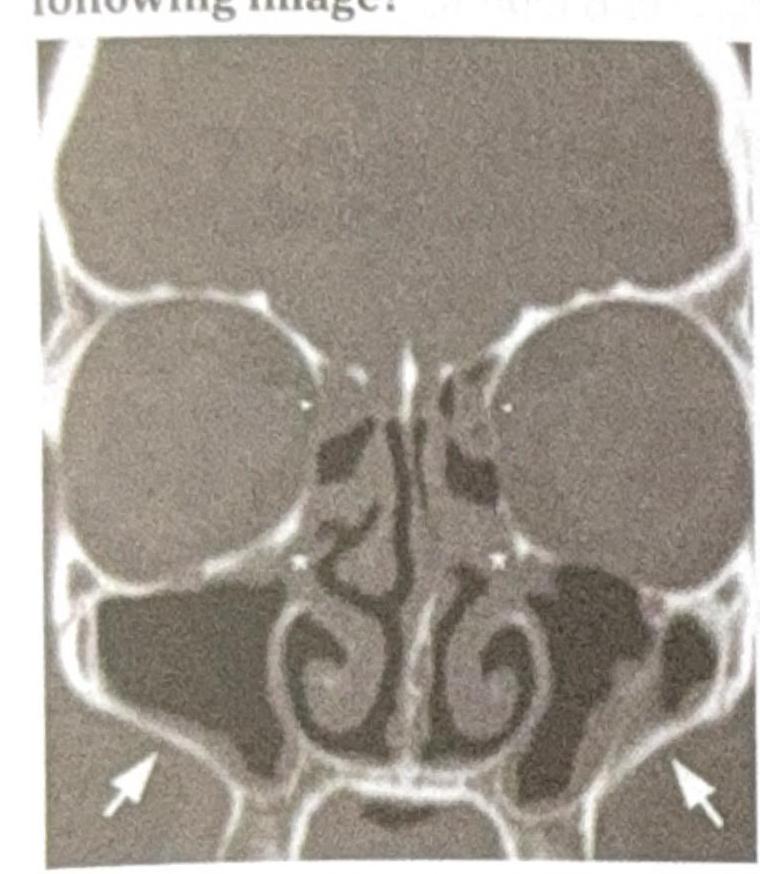
The CT scan of paranasal sinuses shows:
A 65-year-old lady presents with soft swelling on her left supra-orbital area which she says is always warm to touch. She has been taking Ayurvedic treatment for these swellings for the last 6 months. What is the probable diagnosis?

A patient complains of pain and boggy swelling in the frontal region which is warm and tender. He also complains of drowsiness at times. What is the diagnosis?
Which one of the following regarding Nasal polyps is NOT true?
Antro-choanal polyp always arises from:
Pott's puffy tumour is a:
Which sinus drainage is impaired in the following image?
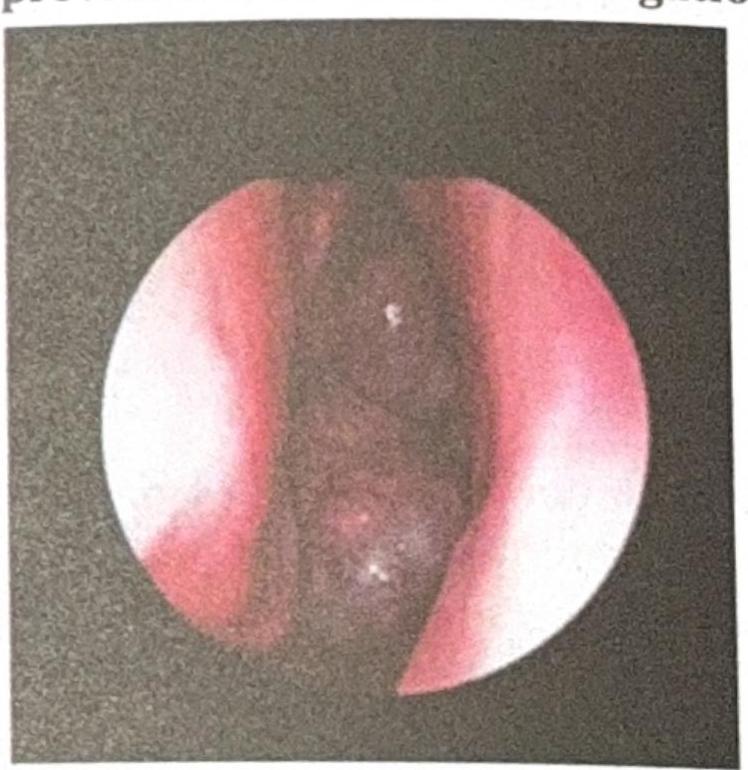
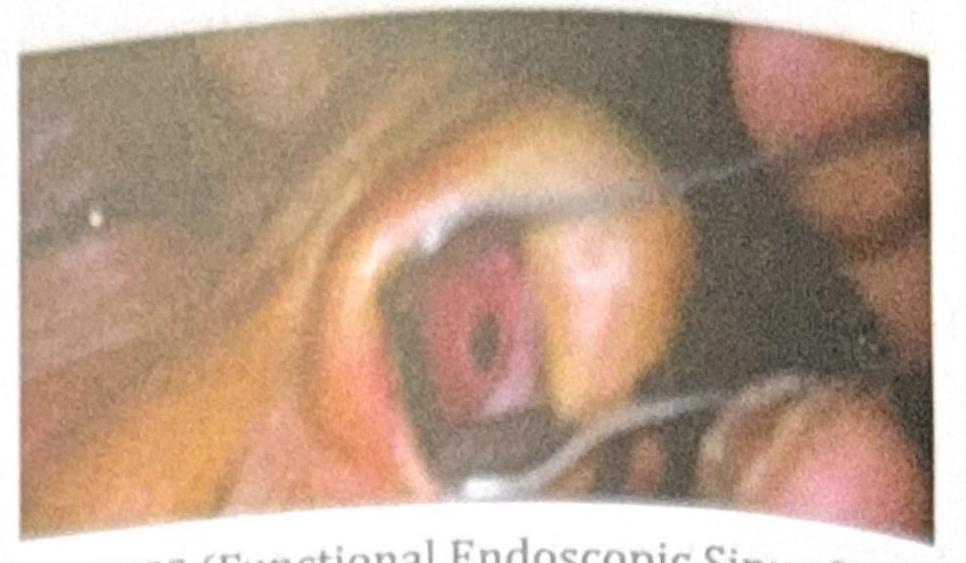
A 14-year-old child with a history of recurrent nasal bleeding has the endoscopic view provided. What is the investigation of choice?
A patient with chronic nasal obstruction underwent a procedure 3 months ago and now presents with recurrent epistaxis, crusting, and the clinical image showing a septal perforation. What procedure was most likely carried out?
A woman visits the ENT outpatient department with complaints of nasal obstruction. On examination, greenish-black crusts were found in the nasal cavity covering the turbinates and septum, and she also had complete anosmia (lack of sense of smell). What other sign is most likely to be found on examination in this case?
Practice by Chapter
Rhinitis
Practice Questions
Acute Rhinosinusitis
Practice Questions
Chronic Rhinosinusitis
Practice Questions
Nasal Polyposis
Practice Questions
Allergic Fungal Sinusitis
Practice Questions
Deviated Nasal Septum
Practice Questions
Epistaxis
Practice Questions
Nasal Trauma
Practice Questions
Choanal Atresia
Practice Questions
CSF Rhinorrhea
Practice Questions
Tumors of the Nose and Paranasal Sinuses
Practice Questions
Complications of Sinusitis
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app