
Diseases of the Nose and Paranasal Sinuses — MCQs

On this page
A patient presents with a thick nasal discharge and headache. Examination reveals hypertrophy of the inferior turbinate with a mulberry appearance. Which of the following is the most likely diagnosis?
A 40-year-old patient presents with recurrent and severe nosebleeds from the anterior nasal septum. The bleeding has been refractory to nasal packing and chemical cautery. A decision is made to proceed with surgical ligation to control the bleeding. Which of the following arteries is the primary target for ligation in the management of this patient's anterior epistaxis?
A patient presents to the emergency department with significant nasal trauma after a fall. Examination reveals a deviated nasal pyramid and palpation confirms crepitus and mobility of the nasal bones. A lateral nasal bone X-ray confirms a displaced nasal bone fracture. Which of the following instruments is specifically designed for the closed reduction of a displaced nasal bone fracture?
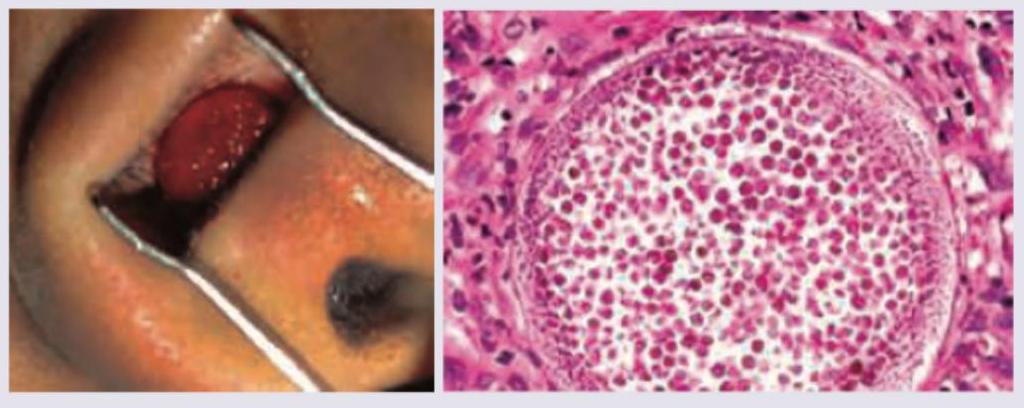
A 15-year-old female presents with nasal obstruction and occasional profuse epistaxis for last 8 weeks. Nasal speculum view and histopathology of resected lesion is given. All are correct about the diagnosis except:
Identify the surgical procedure being performed in the image shown below.
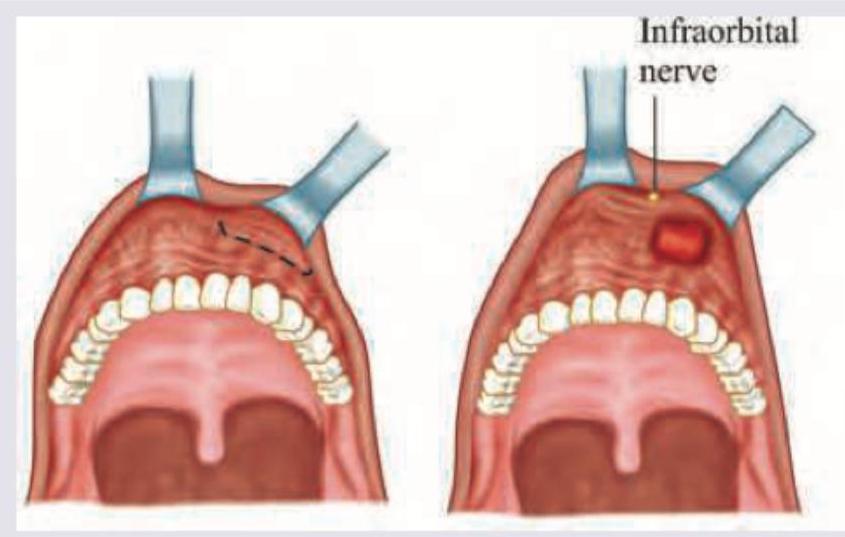
All are contraindications to the procedure shown below except:
An 8-year-old boy presents with recurrent episodes of epistaxis. Histopathological specimen of the excised lesion is shown below. All are correct about this condition except:
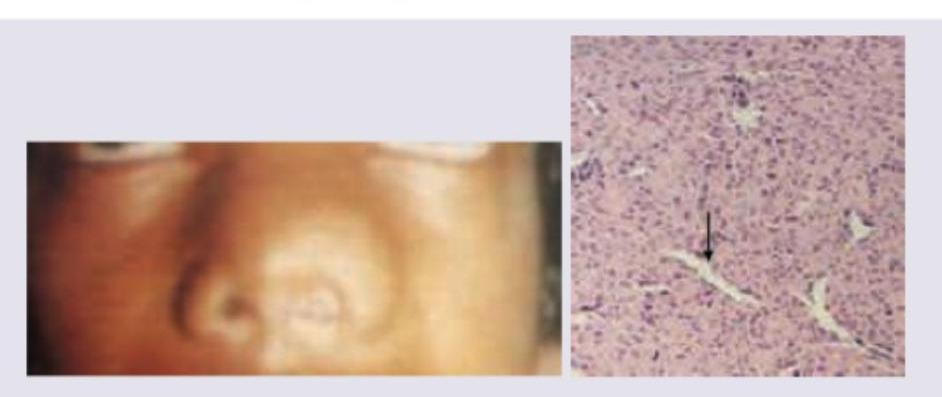
A 10-year-old child is brought with complaints of daily headache and nasal stuffiness. He also has paroxysms of sneezing daily. Nasal examination shows a lesion as shown in the image. All are true about the condition shown except?

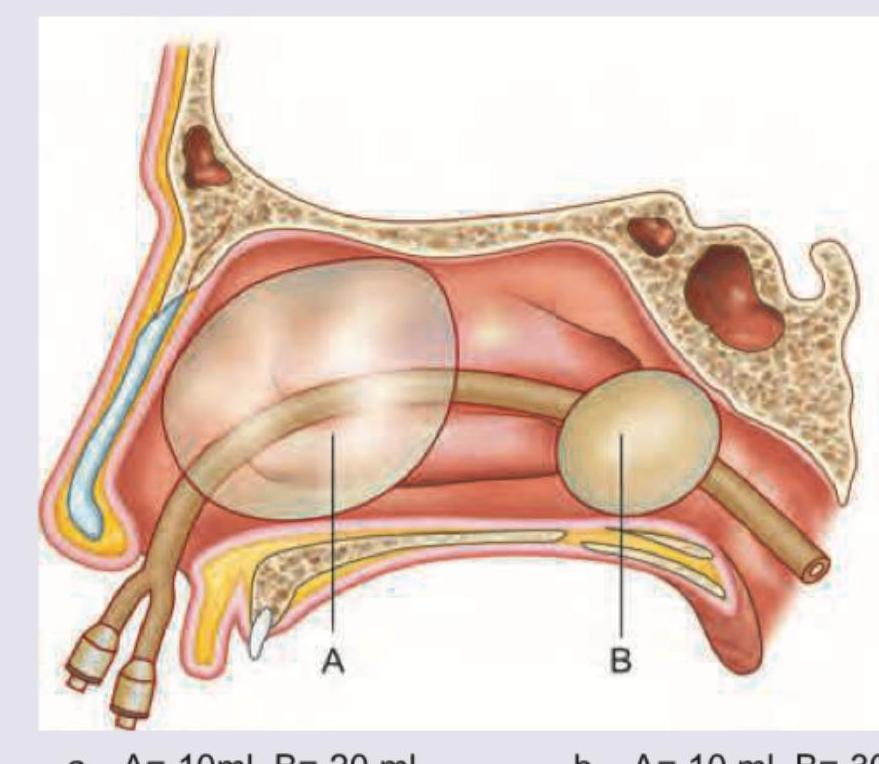
According to the manufacturer specifications for the Epistat double-balloon catheter, what are the recommended inflation volumes for balloons A and B respectively? (Recent NEET Pattern 2016-17)
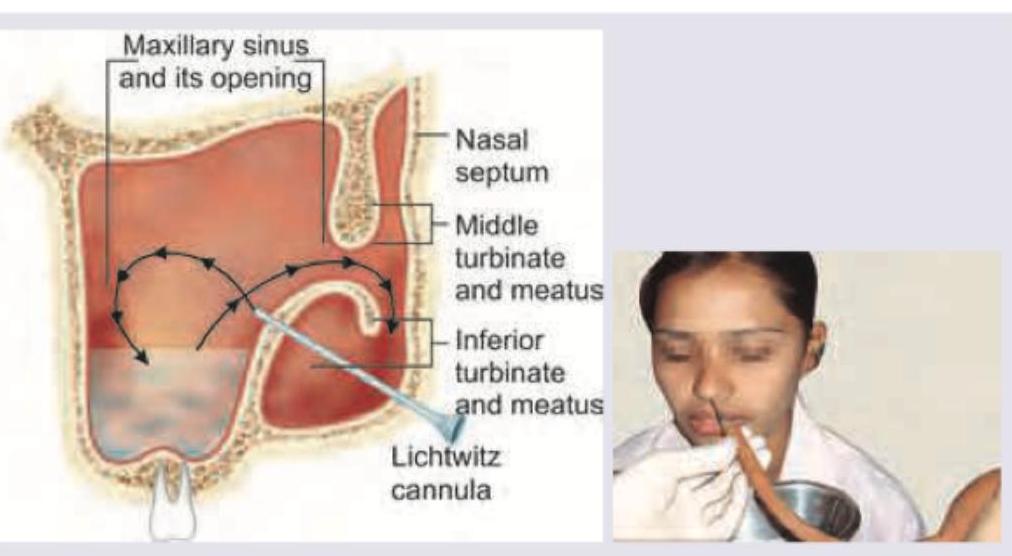
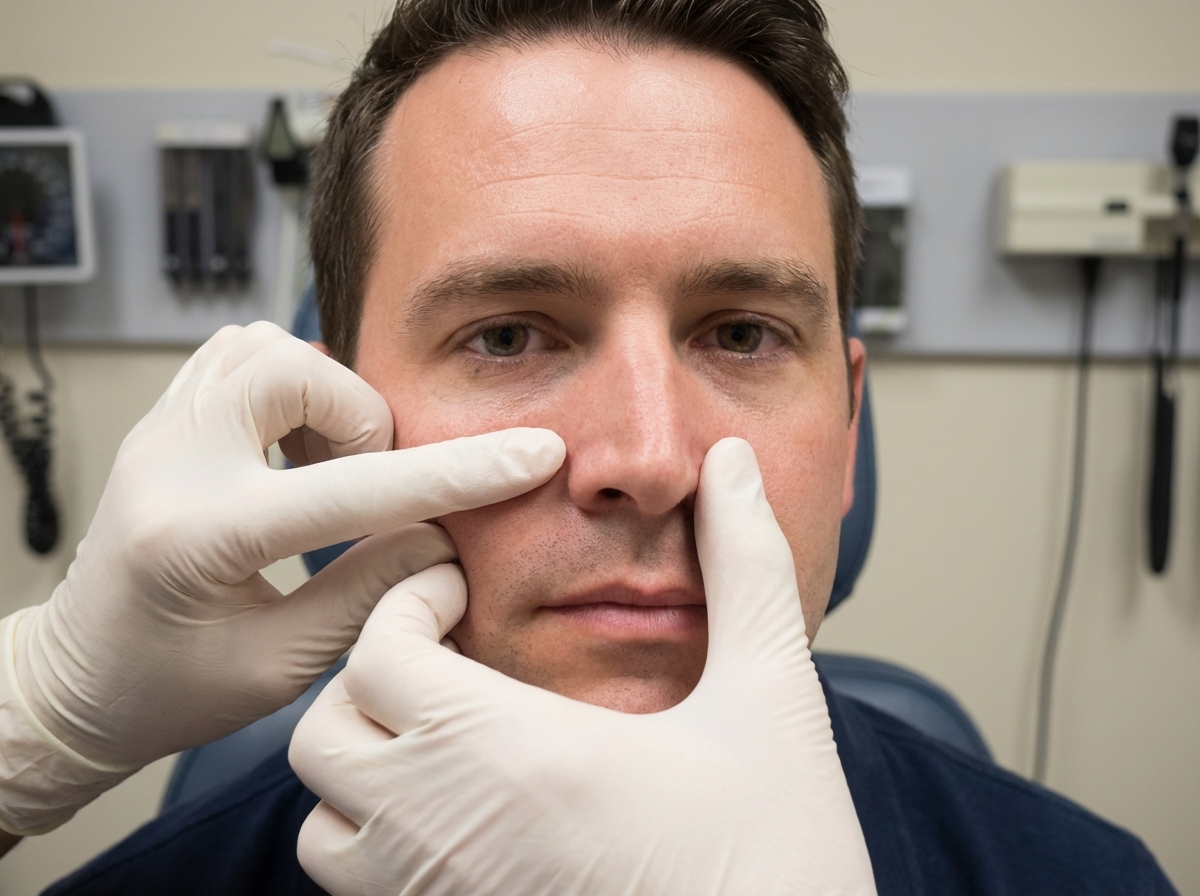
The following test is done for the evaluation of:
Practice by Chapter
Rhinitis
Practice Questions
Acute Rhinosinusitis
Practice Questions
Chronic Rhinosinusitis
Practice Questions
Nasal Polyposis
Practice Questions
Allergic Fungal Sinusitis
Practice Questions
Deviated Nasal Septum
Practice Questions
Epistaxis
Practice Questions
Nasal Trauma
Practice Questions
Choanal Atresia
Practice Questions
CSF Rhinorrhea
Practice Questions
Tumors of the Nose and Paranasal Sinuses
Practice Questions
Complications of Sinusitis
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app