
Diseases of the Nose and Paranasal Sinuses — MCQs

On this page
What is the name of the incision used for the maxillary sinus?
A unilateral mass causing nasal obstruction is seen in the nose of a patient. What is the most probable diagnosis?
What is the diagnosis of a child presenting with a pulsatile swelling on the medial side of the nose?
What is the treatment of choice in bilateral ethmoidal polyps?
A child presents with unilateral, foul smelling nasal discharge. What is the most probable cause?
Following Caldwell-Luc operation, a patient develops hypoesthesia. Which nerve is likely damaged?
Which of the following statements about nasal glioma is FALSE?
A female who underwent laparoscopic appendectomy for acute appendicitis developed difficulty in breathing and a swelling in the anterior part of the nasal septum after bumping her nose on a table on post-operative day 2. What is the next line of management?
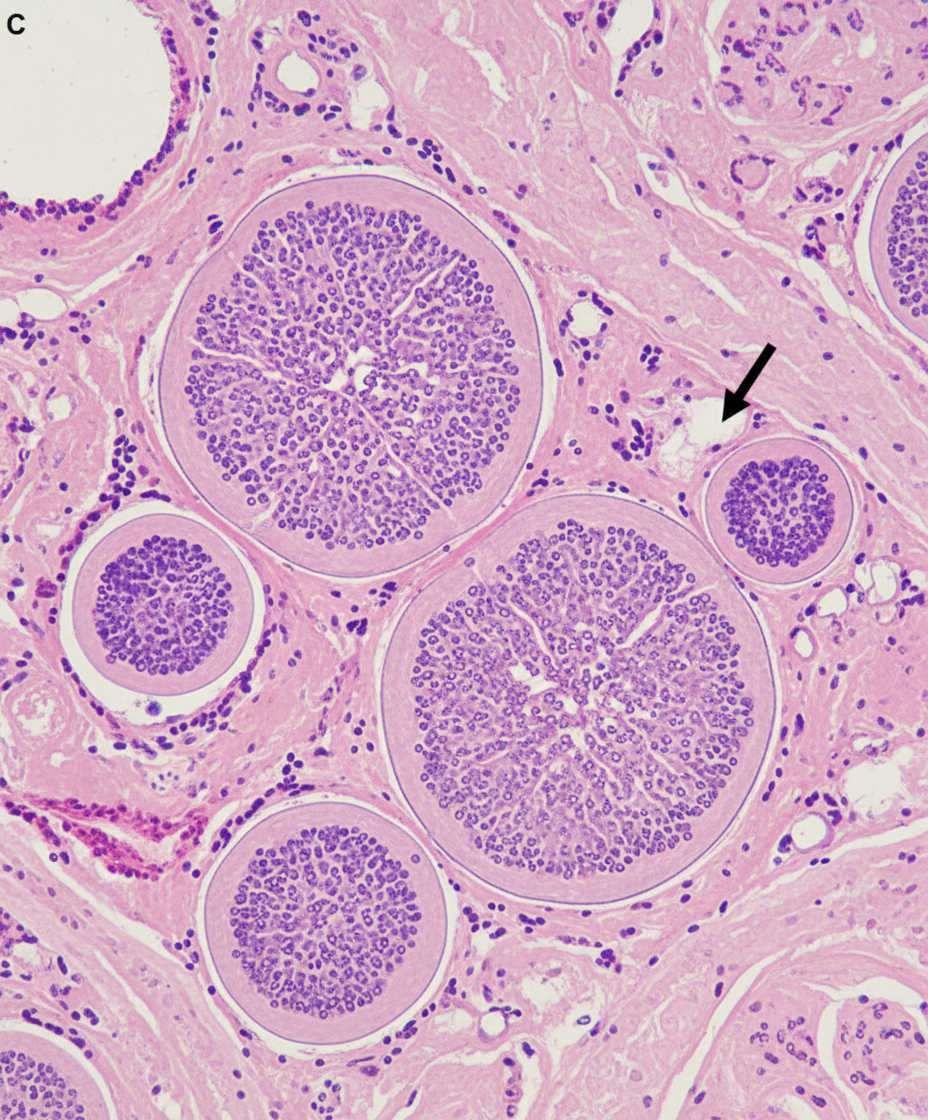
A 60-year-old male complains of right-sided nasal obstruction and nasal discharge, which is sometimes blood-tinged. Biopsy findings are shown below. What is your diagnosis?
A 20-year-old male presents with nasal obstruction and nasal discharge. Nasal endoscopy shows a large polyp in the right nostril extending into the nasopharynx. What is the most appropriate management for this patient?
Practice by Chapter
Rhinitis
Practice Questions
Acute Rhinosinusitis
Practice Questions
Chronic Rhinosinusitis
Practice Questions
Nasal Polyposis
Practice Questions
Allergic Fungal Sinusitis
Practice Questions
Deviated Nasal Septum
Practice Questions
Epistaxis
Practice Questions
Nasal Trauma
Practice Questions
Choanal Atresia
Practice Questions
CSF Rhinorrhea
Practice Questions
Tumors of the Nose and Paranasal Sinuses
Practice Questions
Complications of Sinusitis
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app