
Diseases of the Nose and Paranasal Sinuses — MCQs

On this page
Extraction of a maxillary second molar has resulted in a perforation of the maxillary antrum 0.5 cm in diameter. What is an acceptable procedure?
The nasal mucosa is supplied by which artery?
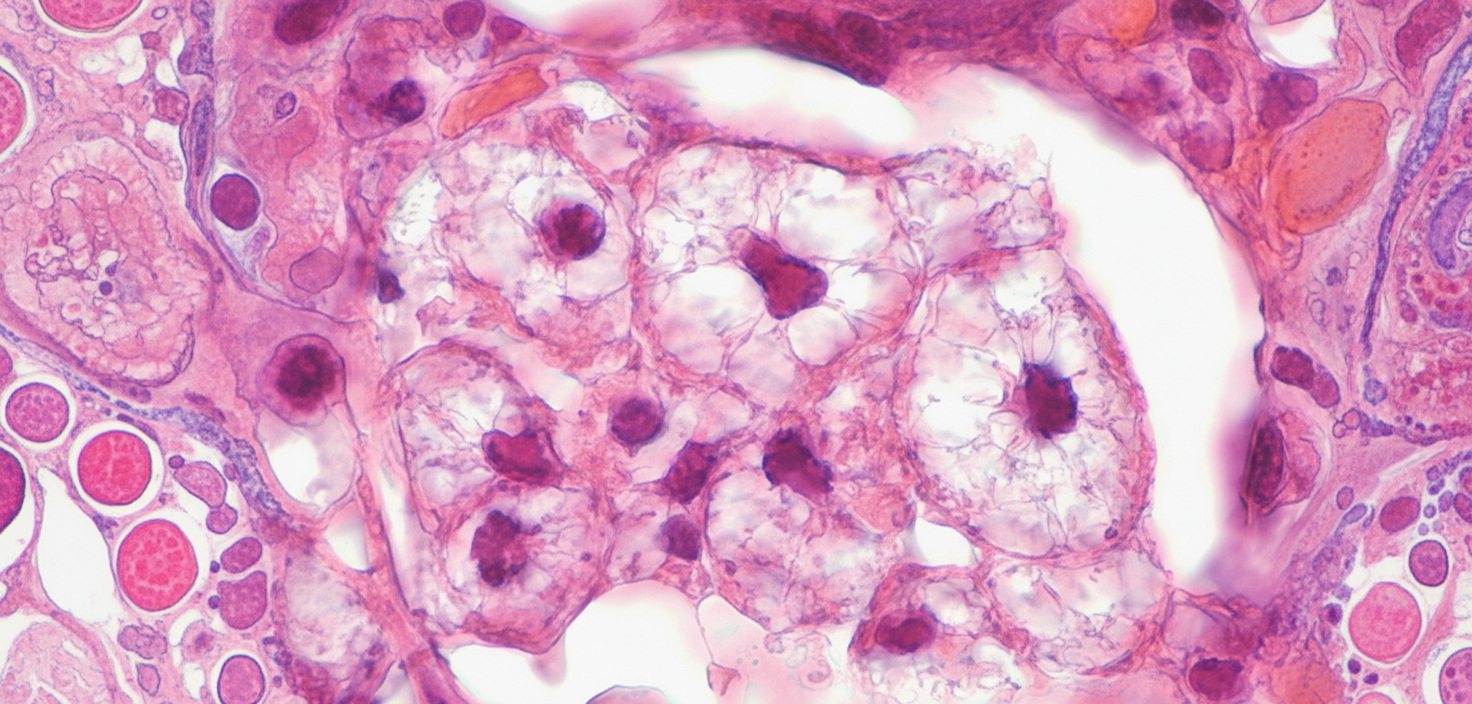
Which of the following statements are true regarding the disease depicted here?
What is the most common cause of unilateral epistaxis in a 5-year-old child?
In a 60-year-old adult, which of the following diseases causes expansile maxillary lesions?
A patient presents with a nasal polypoidal mass and subcutaneous nodules on the skin. What is the most likely diagnosis?
All of the following are true of septoplasty for deviated nasal septum (DNS) except?
Which of the following is common about tumors of the Peripheral Nervous System (PNS) and Nasal Cavity?
Which of the following is used to treat nasal myiasis?
Pott's puffy tumor is related to which of the following conditions?
Practice by Chapter
Rhinitis
Practice Questions
Acute Rhinosinusitis
Practice Questions
Chronic Rhinosinusitis
Practice Questions
Nasal Polyposis
Practice Questions
Allergic Fungal Sinusitis
Practice Questions
Deviated Nasal Septum
Practice Questions
Epistaxis
Practice Questions
Nasal Trauma
Practice Questions
Choanal Atresia
Practice Questions
CSF Rhinorrhea
Practice Questions
Tumors of the Nose and Paranasal Sinuses
Practice Questions
Complications of Sinusitis
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app