
Dermatological Procedures — MCQs

On this page
Which of the following are uses of Wood's light examination?
Tzanck preparation is used for the diagnosis of which of the following skin conditions, EXCEPT?
Complete circumferential and peripheral deep margin assessment is known as:
What is the best treatment for achieving cosmetic results in large port-wine hemangiomas?
Mohs surgery is indicated for which of the following conditions?
What is the wavelength of the carbon dioxide laser?
Microdermabrasion is done with:
The first line treatment for this condition is:
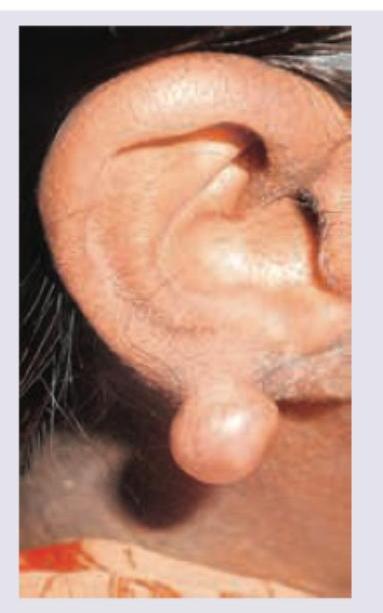
The following image shows:

Best treatment for the lesion shown in the figure?

Practice by Chapter
Skin Biopsy Techniques
Practice Questions
Cryotherapy
Practice Questions
Electrosurgery
Practice Questions
Curettage and Electrodessication
Practice Questions
Excisional Surgery
Practice Questions
Mohs Micrographic Surgery
Practice Questions
Chemical Peels
Practice Questions
Dermabrasion and Microdermabrasion
Practice Questions
Laser Therapy Basics
Practice Questions
Injectable Fillers and Botulinum Toxin
Practice Questions
Photodynamic Therapy
Practice Questions
Wound Care and Dressings
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app