
Dermatological Procedures — MCQs

On this page
Identify the type of skin graft?
Which of the following is NOT true regarding patch testing?
A child presents with erythematous, non-blanching, bosselated lesions on the left side of the face. What is the treatment of choice?
Patch test is done to document which type of hypersensitivity?
All of the following are used in cryosurgery except?
What is the wavelength of light produced by a Wood's lamp?
Which of the following is not an agent used in chemical peeling?
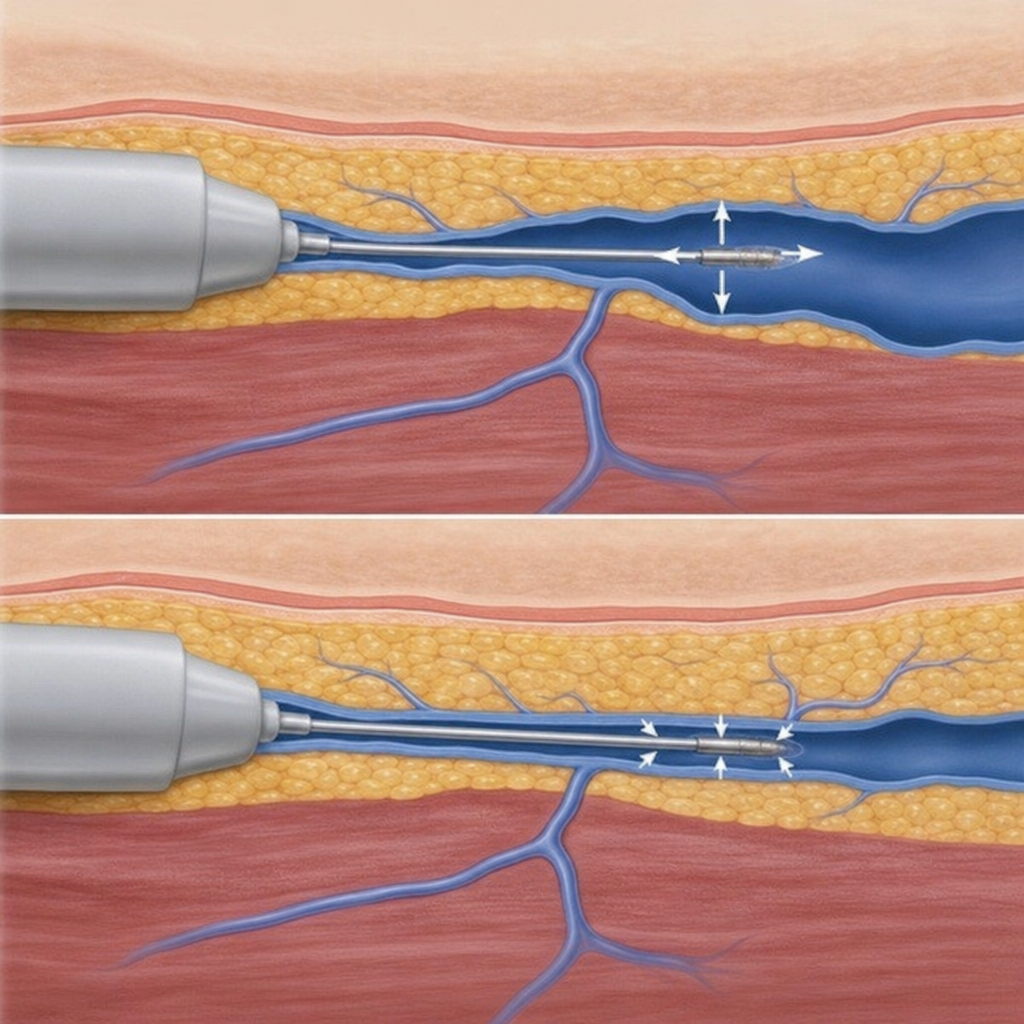
What is the mechanism by which the following technique works?
Mohs micrographic excision for basal cell carcinoma is used for all of the following indications except:
Tzanck preparation is used for the diagnosis of which of the following skin conditions, EXCEPT?
Practice by Chapter
Skin Biopsy Techniques
Practice Questions
Cryotherapy
Practice Questions
Electrosurgery
Practice Questions
Curettage and Electrodessication
Practice Questions
Excisional Surgery
Practice Questions
Mohs Micrographic Surgery
Practice Questions
Chemical Peels
Practice Questions
Dermabrasion and Microdermabrasion
Practice Questions
Laser Therapy Basics
Practice Questions
Injectable Fillers and Botulinum Toxin
Practice Questions
Photodynamic Therapy
Practice Questions
Wound Care and Dressings
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app