
Bacterial Skin Infections — MCQs

On this page
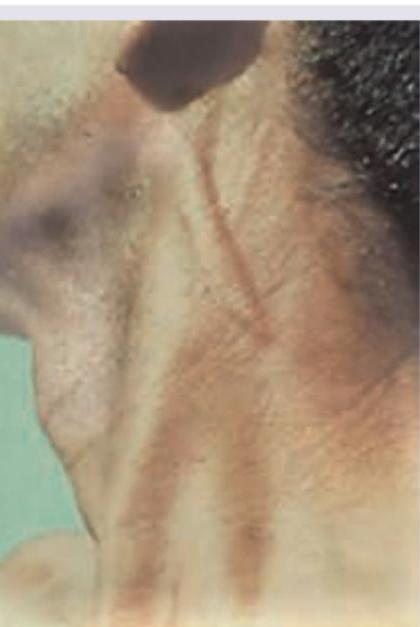
Which nerve is thickened in this patient of Hansen disease?
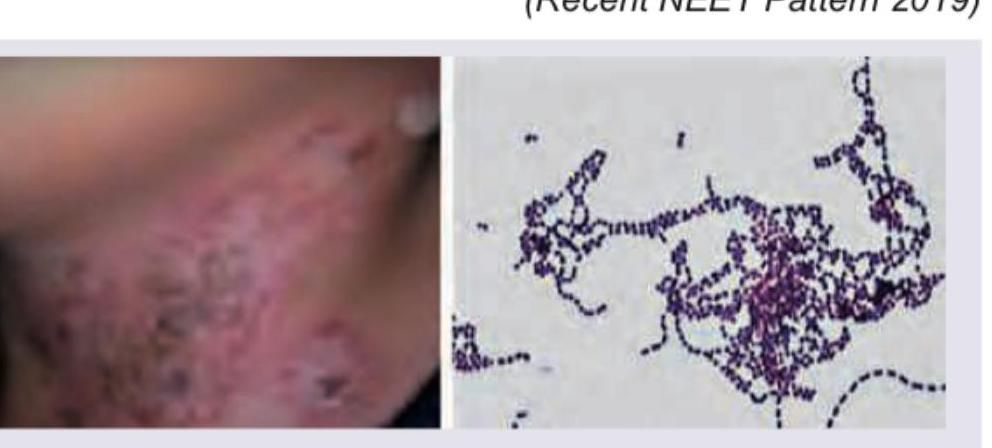
A child presents with an asymptomatic, well-demarcated, finely scaly reddish-brown plaque in a neck fold, as shown. The lesion demonstrates coral-red fluorescence on Wood-lamp examination, and Gram-positive bacilli are identified. What is the diagnosis?
Which one of the following statements is correct regarding leprosy?
With reference to lepromin test, which one of the following statements is correct?
The characteristic features of inguinal lymph nodes associated with a primary syphilitic lesion of the vulva are
Painless genital ulcer is found in which one of the following genital infections?
A woman presents with heavy foul smelling discharge with sharply demarcated ulcers without induration on the perineum and the labia majora. Inguinal lymphadenopathy is also present. What is the most probable diagnosis?
A 45-year-old man presents with a 3-month history of progressive, painless ulcerative lesions on his penis and scrotum. He has no systemic symptoms. Laboratory tests show negative HIV, negative VDRL and TPHA, and negative HSV PCR. Biopsy shows pseudoepitheliomatous hyperplasia with plasma cells and macrophages containing intracytoplasmic organisms. What is the most likely diagnosis?
A 30-year-old woman is diagnosed with gonorrhea and reports a penicillin allergy (rash). Which alternative treatment regimen is most appropriate?
Which of the following is NOT characteristic of lymphogranuloma venereum proctitis?
Practice by Chapter
Impetigo
Practice Questions
Folliculitis, Furuncles, and Carbuncles
Practice Questions
Ecthyma
Practice Questions
Erysipelas and Cellulitis
Practice Questions
Staphylococcal Scalded Skin Syndrome
Practice Questions
Necrotizing Fasciitis
Practice Questions
Cutaneous Tuberculosis
Practice Questions
Leprosy
Practice Questions
Lyme Disease
Practice Questions
Syphilis
Practice Questions
Antibiotic Resistance in Dermatology
Practice Questions
Prophylaxis and Management
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app