
Bacterial Skin Infections — MCQs

On this page
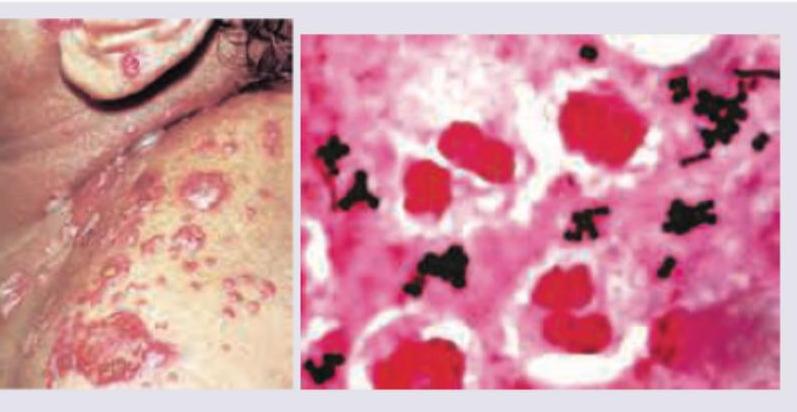
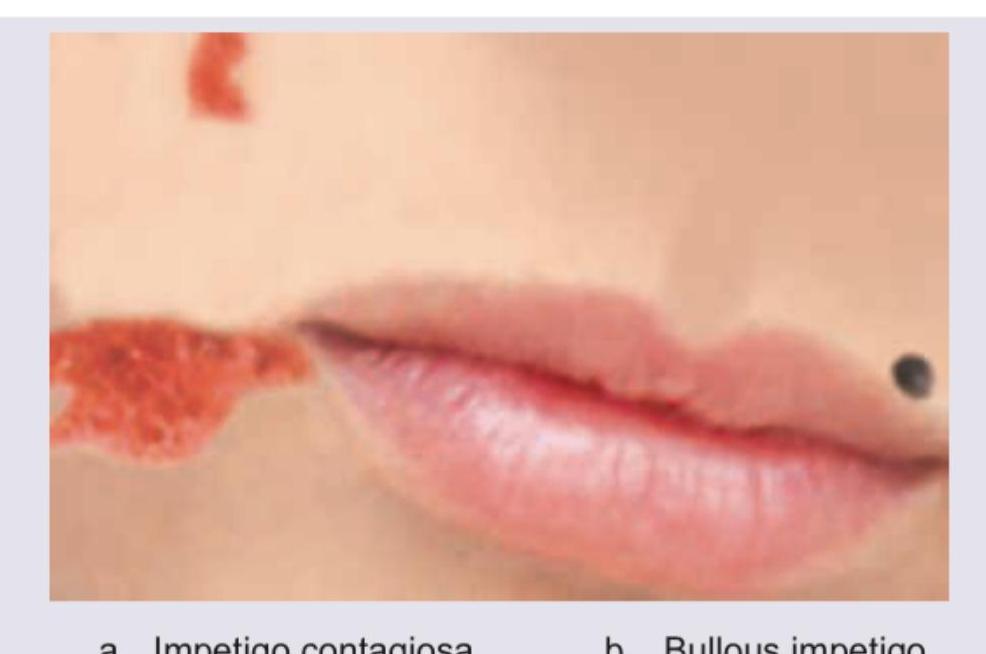
All are correct about the condition shown in the image except: (Recent NEET Pattern 2016-17)

A child presents with skin lesions that started as vesicles that enlarged into flaccid bullae, which ruptured leaving annular erosions with peripheral collarettes. A Gram stain of the lesion shows Gram-positive cocci in clusters. The diagnosis is:
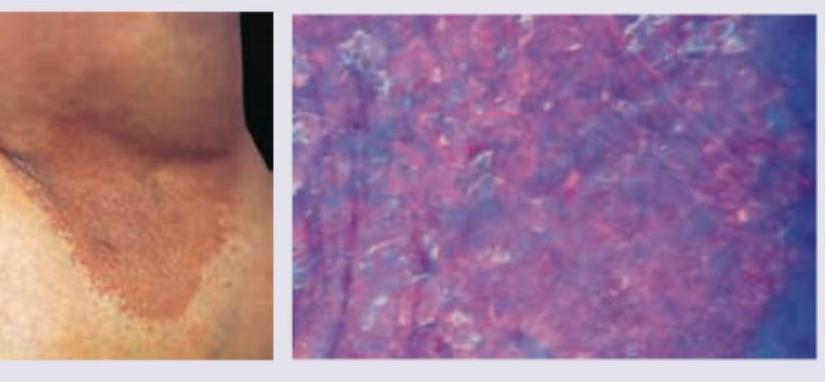
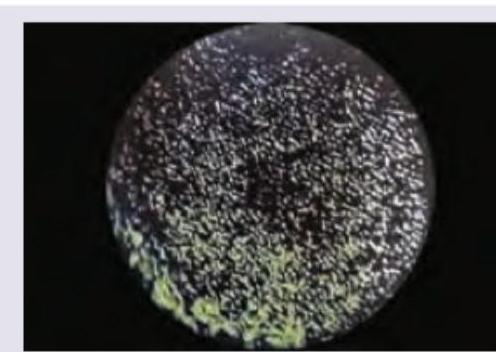
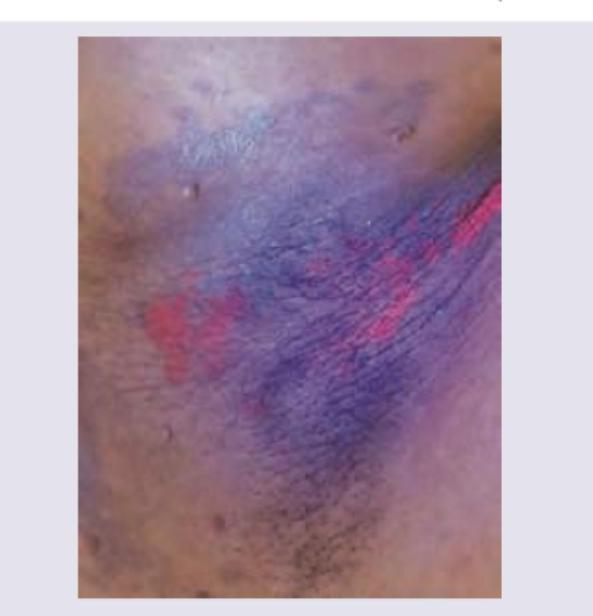
A 35-year-old obese woman presents with recurrent lesions in both axilla in summer season. Wood lamp examination is shown. The diagnosis is:
The following image is diagnostic of which STD?

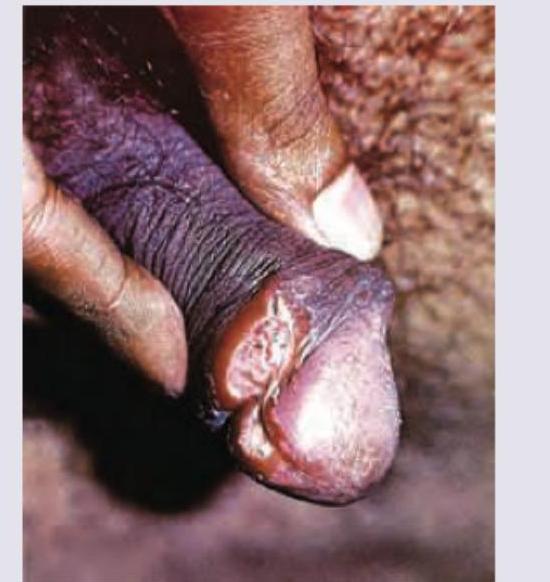
A 30-year-old male patient presents with painful genital lesion after unprotected sexual intercourse. He is non cooperative during genital manipulation done to take culture specimen. All are true about the condition shown except:
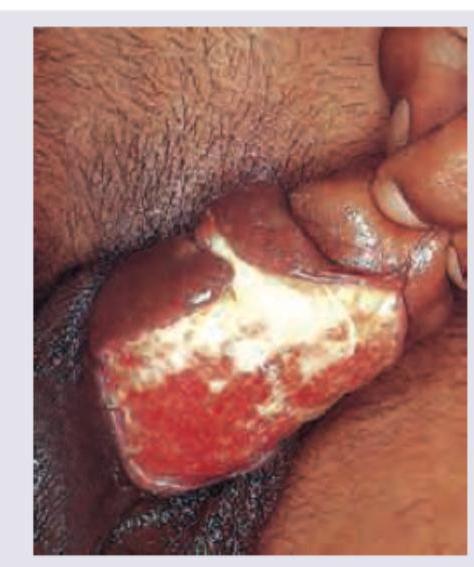
A patient presents with a genital lesion that has been slowly progressive over several weeks. The lesion is painless, bleeds easily on contact, and there is no associated inguinal lymphadenopathy. What is the diagnosis based on the image and clinical findings shown below?
A 25-year-old woman presents with skin lesion on left supra-orbital margin. Eye examination is within normal limits. CXR done was normal. Diascopy shows apple jelly nodules. The image shows presence of:

A child presents with the skin lesions shown in the image. The most likely diagnosis is:
A patient presents with discoloration and dystrophy of the fingernail. The following appearance under Wood's lamp examination of the affected nail is seen in:
The following appearance on Wood's lamp is seen in?
Practice by Chapter
Impetigo
Practice Questions
Folliculitis, Furuncles, and Carbuncles
Practice Questions
Ecthyma
Practice Questions
Erysipelas and Cellulitis
Practice Questions
Staphylococcal Scalded Skin Syndrome
Practice Questions
Necrotizing Fasciitis
Practice Questions
Cutaneous Tuberculosis
Practice Questions
Leprosy
Practice Questions
Lyme Disease
Practice Questions
Syphilis
Practice Questions
Antibiotic Resistance in Dermatology
Practice Questions
Prophylaxis and Management
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app