
Bacterial Skin Infections — MCQs

On this page
All are the characteristics of cellulitis, EXCEPT?
The Ridley-Jopling classification for leprosy is based on which of the following parameters?
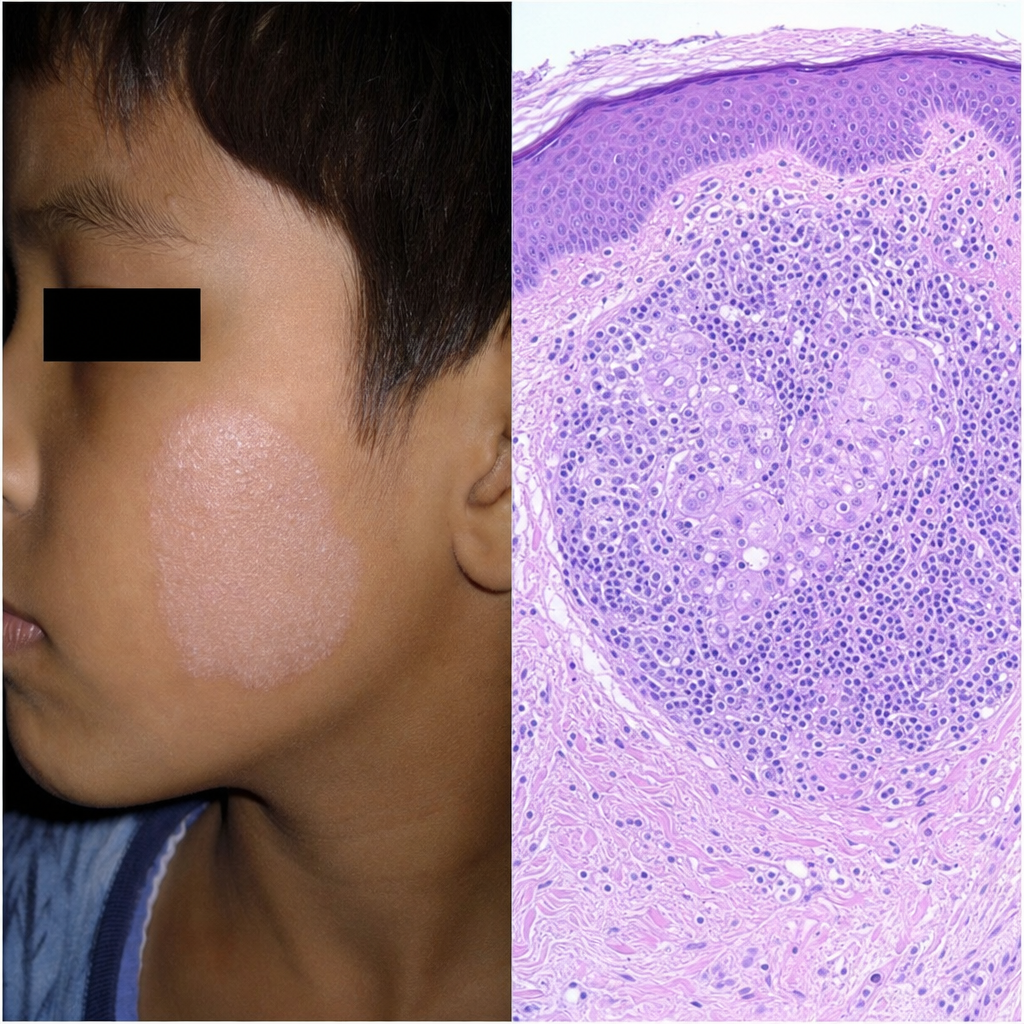
A child presents with a facial lesion, as depicted in the accompanying image. A biopsy of the lesion is also shown. What is the most probable diagnosis?
Which of the following tuberculides is characterized by involvement of sweat glands and hair follicles with non-caseating epithelioid granuloma?
Which of the following conditions does not involve nerve damage?
True about Lucio's phenomenon is:
Tuberculides are seen in which of the following conditions?
Multidrug therapy is indicated for which of the following conditions?
What is the treatment for Lucio phenomenon?
Which of the following can lead to infiltration of ear lobules, loss of nails, and resorption of distal phalanges?
Practice by Chapter
Impetigo
Practice Questions
Folliculitis, Furuncles, and Carbuncles
Practice Questions
Ecthyma
Practice Questions
Erysipelas and Cellulitis
Practice Questions
Staphylococcal Scalded Skin Syndrome
Practice Questions
Necrotizing Fasciitis
Practice Questions
Cutaneous Tuberculosis
Practice Questions
Leprosy
Practice Questions
Lyme Disease
Practice Questions
Syphilis
Practice Questions
Antibiotic Resistance in Dermatology
Practice Questions
Prophylaxis and Management
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app