
Bacterial Skin Infections — MCQs

On this page
A truck driver presents with a single painless genital ulcer that appeared 3 weeks after an unprotected sexual encounter. There is associated non-tender inguinal lymphadenopathy. What is the most likely diagnosis?
A patient presents with multiple painful genital ulcers associated with tender cervical/inguinal lymphadenopathy. The ulcers are soft and irregular as shown in the image. What is the most likely causative organism?
A female presents with greenish frothy discharge; whiff test and Amsel’s criteria are negative. What microscopy feature is expected?
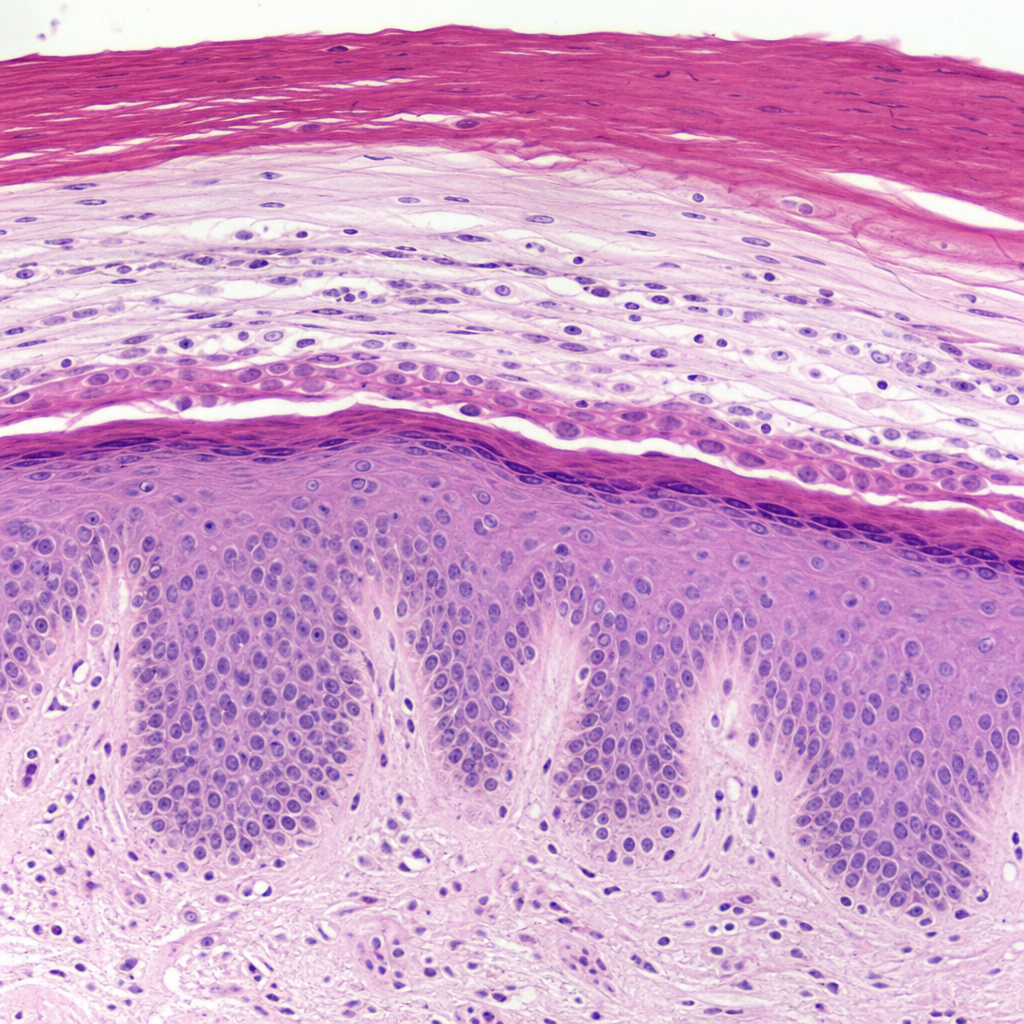
A 38-year-old man with a known history of well-controlled plaque psoriasis on his elbows and knees presents for a routine review. He mentions his nails have become unsightly and occasionally painful. Examination of the hands is performed and the findings are shown (Image 3). Which histopathological finding in the nail unit is most directly responsible for the proximal nail plate changes visible in this image?
A patient presents with multiple hypopigmented and hypesthetic patches on the lateral aspect of the forearm, with abundant acid-fast bacilli (AFB) and granulomatous inflammation on histology. What is the most likely diagnosis?
What is the worldwide accepted minimum dose of penicillin for latent syphilis?
Which subtype of leprosy has the maximum number of TH1 cells?
A young boy has a single scaly, hypoanaesthetic patch over the hand plus thickened ulnar nerve. What is the diagnosis?
What is most important in establishing the diagnosis of leprosy?
Milian's ear sign is seen in which of the following conditions?
Practice by Chapter
Impetigo
Practice Questions
Folliculitis, Furuncles, and Carbuncles
Practice Questions
Ecthyma
Practice Questions
Erysipelas and Cellulitis
Practice Questions
Staphylococcal Scalded Skin Syndrome
Practice Questions
Necrotizing Fasciitis
Practice Questions
Cutaneous Tuberculosis
Practice Questions
Leprosy
Practice Questions
Lyme Disease
Practice Questions
Syphilis
Practice Questions
Antibiotic Resistance in Dermatology
Practice Questions
Prophylaxis and Management
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app