
Epidemiology — MCQs

On this page
A community health center is developing a comprehensive program that includes vaccination campaigns, screening for hypertension and diabetes, and rehabilitation services for stroke survivors. Which levels of prevention are being addressed by this program?
A new mammography technique has 95% sensitivity and 88% specificity for breast cancer detection. The current standard has 85% sensitivity and 95% specificity. Both techniques cost the same to implement. Which approach would be most appropriate for a national screening program?
A diagnostic test for a rare disease has 99% sensitivity and 95% specificity. In a population with 0.1% disease prevalence, analyze the clinical utility of this test for screening purposes.
A diagnostic test for COVID-19 has 95% sensitivity and 98% specificity. In a community with 2% prevalence, analyze the implications of implementing this test for mass screening versus using it for symptomatic patients only.
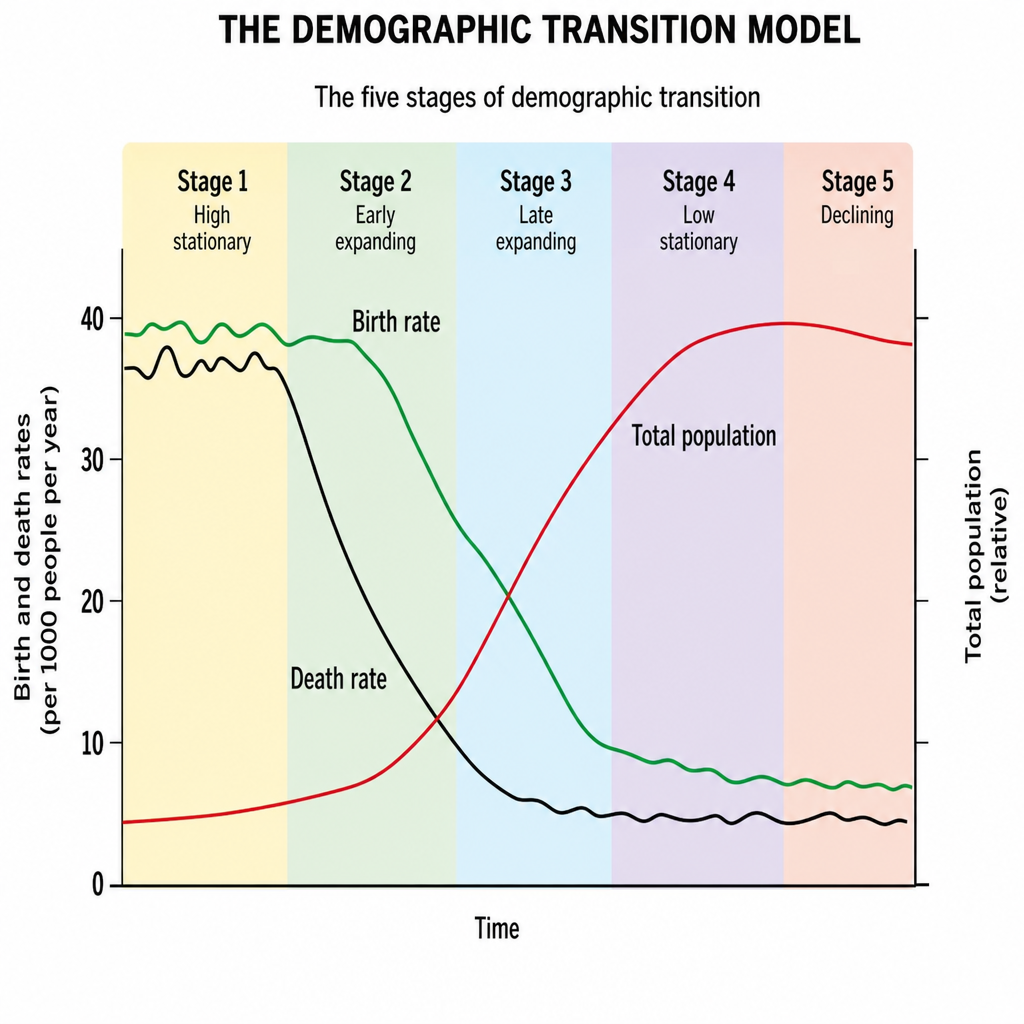
In demographic transition analysis, what does the difference between birth rates and death rates represent when plotting demographic changes over time?
What is the period called between the entry of an organism into the host and the point of maximum infectivity?
The incubation period of a disease is 5-14 days. What should be the quarantine period?
The Black Line in the demographic cycle represents:
Which of the following diseases has the largest submerged portion in the iceberg model of disease?
Which of the following is a true statement about screening tests for genetic diseases?
Practice by Chapter
Principles of Epidemiology
Practice Questions
Measures of Disease Frequency
Practice Questions
Epidemiological Study Designs
Practice Questions
Descriptive Epidemiology
Practice Questions
Analytical Epidemiology
Practice Questions
Experimental Epidemiology
Practice Questions
Screening for Disease
Practice Questions
Surveillance Systems
Practice Questions
Investigation of an Epidemic
Practice Questions
Association and Causation
Practice Questions
Modern Epidemiological Methods
Practice Questions
Critical Appraisal of Epidemiological Studies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app