
Epidemiology — MCQs

On this page
Standardized Mortality ratio is best explained by which one of the following statements?
Which one of the following statements is NOT true for taking a decision on screening for disease?
The sequence of events leading to disability and handicap is:
Physical Quality of life consolidates which of the following indicators? 1. Infant Mortality Rate 2. Life expectancy at birth 3. Literacy 4. Per capita income 5. Mean years of schooling 6. Life expectancy at age one Select the correct answer using the code given below:
Disability-adjusted life years (DALYs) include:
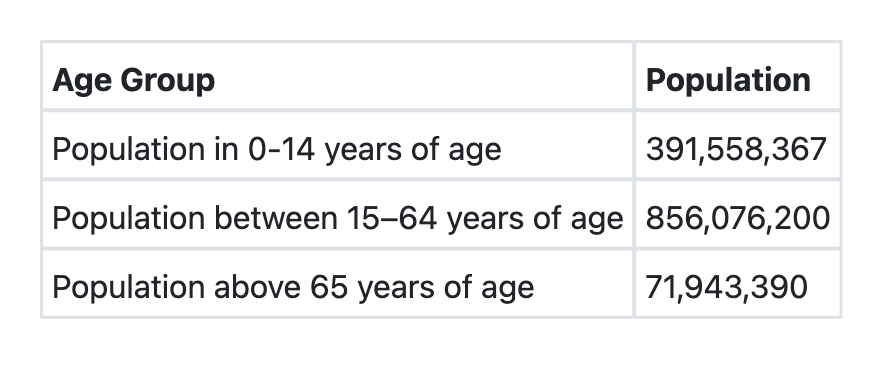
Consider the following data for a country: What shall be the dependency ratio of this country?
Which one of the following is NOT a function of Epidemiology?
In a cohort of 500 women attending antenatal clinic, 70 % had ultrasonography (USG). This cohort was followed up at delivery. Of the women who had USG, 70 delivered low birth weight (LBW) babies; whereas of the women, who did not undergo USG, 50 delivered LBW babies. The incidence of LBW babies among women who had USG is:
Poor hand hygiene of a mess worker in a university college mess led to Hepatitis A cases in the hostel inmates. What type of epidemic will this exposure present with? 1. Propagated 2. Common source-continuous exposure 3. Common source-point exposure Select the correct answer using the code given below:
Keeping biological determinants in perspective, consider the following statements: 1. Presence of a normal karyotype is the first requisite for human health 2. Genetic screening can play an important role in prevention of wide spectrum of diseases 3. If an individual is allowed to live in healthy relationship with the environment, the person's genetic potentialities can transform into phenotypic realities Which of the above statements is/are correct?
Practice by Chapter
Principles of Epidemiology
Practice Questions
Measures of Disease Frequency
Practice Questions
Epidemiological Study Designs
Practice Questions
Descriptive Epidemiology
Practice Questions
Analytical Epidemiology
Practice Questions
Experimental Epidemiology
Practice Questions
Screening for Disease
Practice Questions
Surveillance Systems
Practice Questions
Investigation of an Epidemic
Practice Questions
Association and Causation
Practice Questions
Modern Epidemiological Methods
Practice Questions
Critical Appraisal of Epidemiological Studies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app