
Epidemiology — MCQs

On this page
The pattern of disease in a community described in terms of the important factors which influence its occurrence is known as:
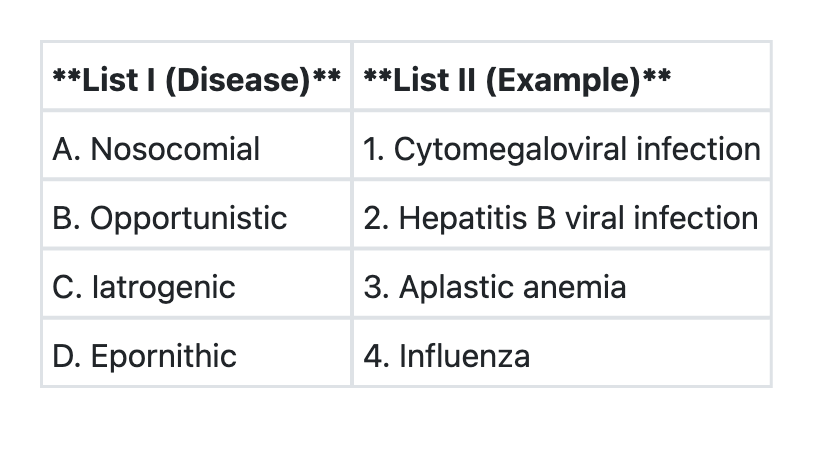
Match List I with List II and select the correct answer using the codes given below the lists:
Which of the following statements is/are true about proportional case rate of malaria? 1. This indicator is used since morbidity rate is difficult to determine 2. This is defined as the number of cases of malaria for every 100 patients seen in hospital OPDs 3. It is a crude index since cases are not related to their time and space distribution Select the correct answer using the code given below:
With reference to mumps, consider the following statements: 1. The average age of incidence of mumps is higher than that of measles and chicken pox. 2. The mumps disease tends to be more severe in adults than in children. Which of the statements given above is/are correct?
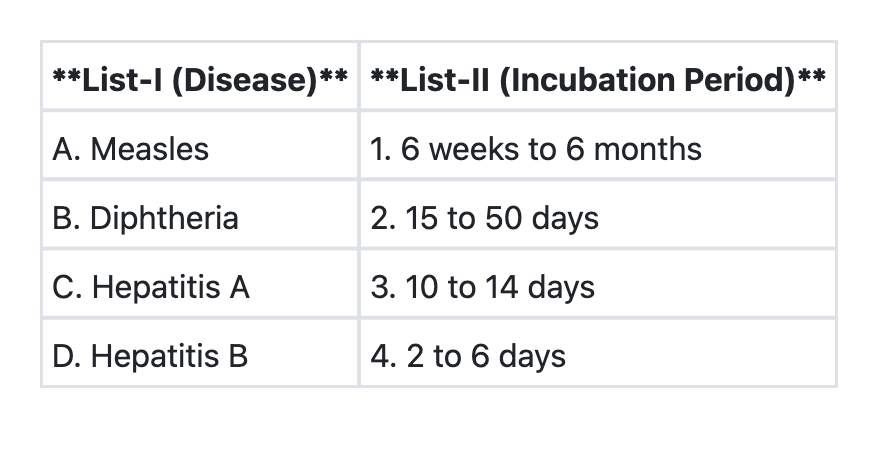
Match List-I with List-II and select the correct answer using the code given below the Lists:
Chemoprophylaxis is an example of:
The most sensitive indicator of the health status of a community is the:
Sullivan Index is the measure of which of the following?
The time period from entry of an infective agent into a host until the host develops the capacity for maximal infectivity is called:
In a family of six (2 parents and 4 children), the youngest child catches measles infection. The parents are immune to the infection. On 3rd and 5th day of the infection of the first child, the two other children also suffer from measles. The secondary attack rate (SAR) of measles is:
Practice by Chapter
Principles of Epidemiology
Practice Questions
Measures of Disease Frequency
Practice Questions
Epidemiological Study Designs
Practice Questions
Descriptive Epidemiology
Practice Questions
Analytical Epidemiology
Practice Questions
Experimental Epidemiology
Practice Questions
Screening for Disease
Practice Questions
Surveillance Systems
Practice Questions
Investigation of an Epidemic
Practice Questions
Association and Causation
Practice Questions
Modern Epidemiological Methods
Practice Questions
Critical Appraisal of Epidemiological Studies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app