
Epidemiology — MCQs

On this page
Which of the following Screening methods for Disease is the least useful?
What constitutes the denominator in ‘Total Dependency Ratio’?
Which of the following is/are suggested by rising incidence rates of any disease? 1. Need for a new disease control programme 2. Improvement in reporting practices 3. Change in the etiology of the disease Select the correct answer using the codes given below:
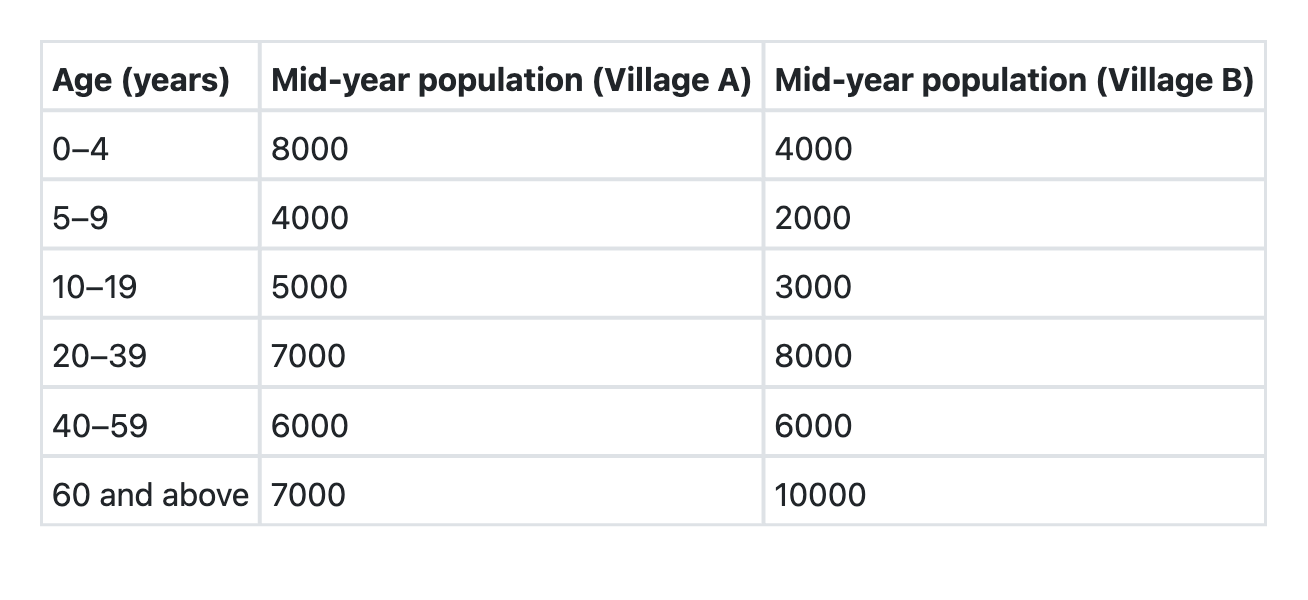
The villages A and B have the following age compositions: Which of the following is the best indicator for comparing the death rates of these two villages?
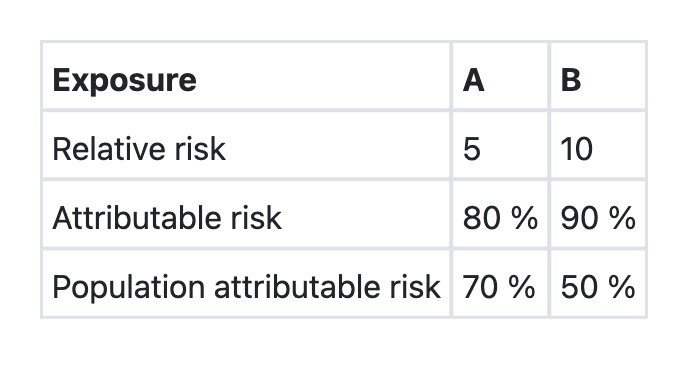
The data regarding two exposures A and B, associated with a disease X in a community is given below: Which one of the following assertions and the reasons given is correct?
Asymptomatic carriers of pathogenic organisms are called:
A well of contaminated water resulted in an outbreak of diarrhoea in a community. Which type of epidemic will this exposure present with? 1.Propagated epidemic 2.Common source - continuous exposure 3.Common source - point exposure
The yield of a screening test CAN NOT be increased by which of the following?
What are the characteristics of ideal health indicators?
After attending a birthday party in a hostel around 50 students reported having loose stools, fever and a few reported vomiting. This outbreak can be identified as what type of outbreak ?
Practice by Chapter
Principles of Epidemiology
Practice Questions
Measures of Disease Frequency
Practice Questions
Epidemiological Study Designs
Practice Questions
Descriptive Epidemiology
Practice Questions
Analytical Epidemiology
Practice Questions
Experimental Epidemiology
Practice Questions
Screening for Disease
Practice Questions
Surveillance Systems
Practice Questions
Investigation of an Epidemic
Practice Questions
Association and Causation
Practice Questions
Modern Epidemiological Methods
Practice Questions
Critical Appraisal of Epidemiological Studies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app