
Epidemiology — MCQs

On this page
Secular trends of diseases refer to
In which system, continuous enumeration of births and deaths by enumerator and an independent survey by investigator supervisor is done?
Other than cataract, which one among the following is the highest prevalent cause of blindness in the world ?
The law stating that "the relative frequencies of each gene allele tend to remain constant from generation to generation" is known as
Which one of the following is a correct combination regarding Indian population?
Amniocentesis in early pregnancy for genetic disorders is a kind of
The period of time required for the development of the parasite from the gametocyte to sporozoite stage in the body of the mosquito is about 10-20 days. This period is also referred to as
In a community with one lakh population, 20,000 slides were examined in a particular year. Out of these 100 were positive for malarial parasite. What is the Annual Parasite Incidence (API) in this community ?
Berksonian bias is a selection bias which occurs in
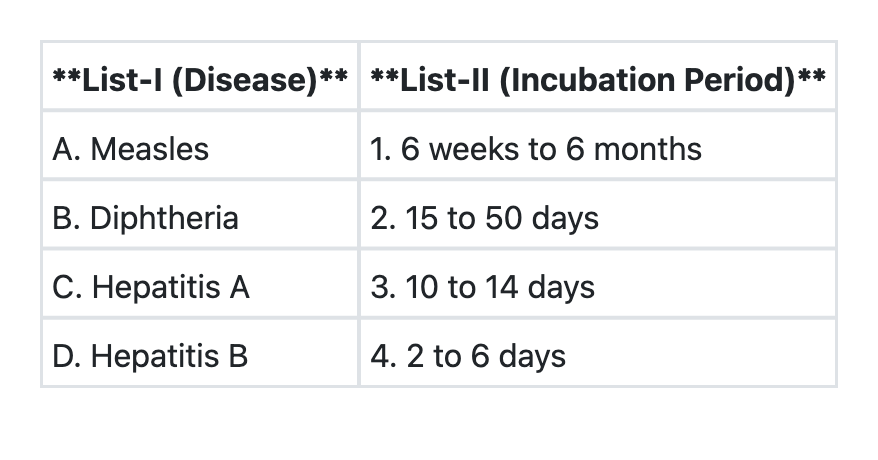
Match the diseases in List-I with their respective incubation periods in List-II and select the correct answer using the code given below:
Practice by Chapter
Principles of Epidemiology
Practice Questions
Measures of Disease Frequency
Practice Questions
Epidemiological Study Designs
Practice Questions
Descriptive Epidemiology
Practice Questions
Analytical Epidemiology
Practice Questions
Experimental Epidemiology
Practice Questions
Screening for Disease
Practice Questions
Surveillance Systems
Practice Questions
Investigation of an Epidemic
Practice Questions
Association and Causation
Practice Questions
Modern Epidemiological Methods
Practice Questions
Critical Appraisal of Epidemiological Studies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app