
Epidemiology — MCQs

On this page
What does the given image show?
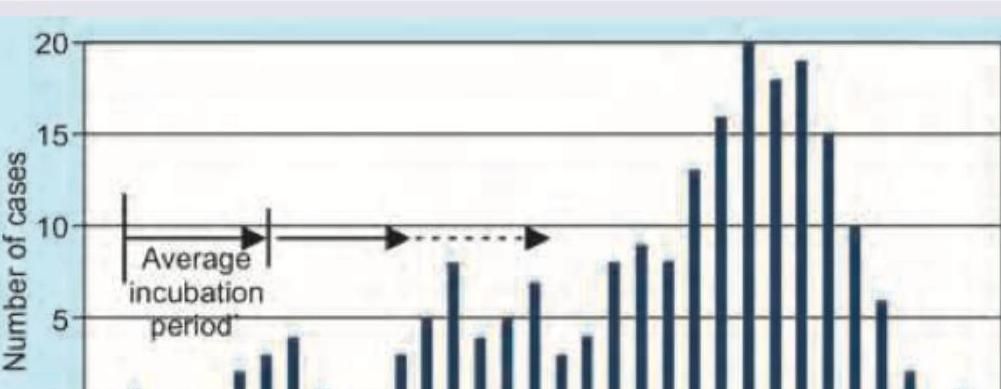
The given image shows which kind of epidemic?
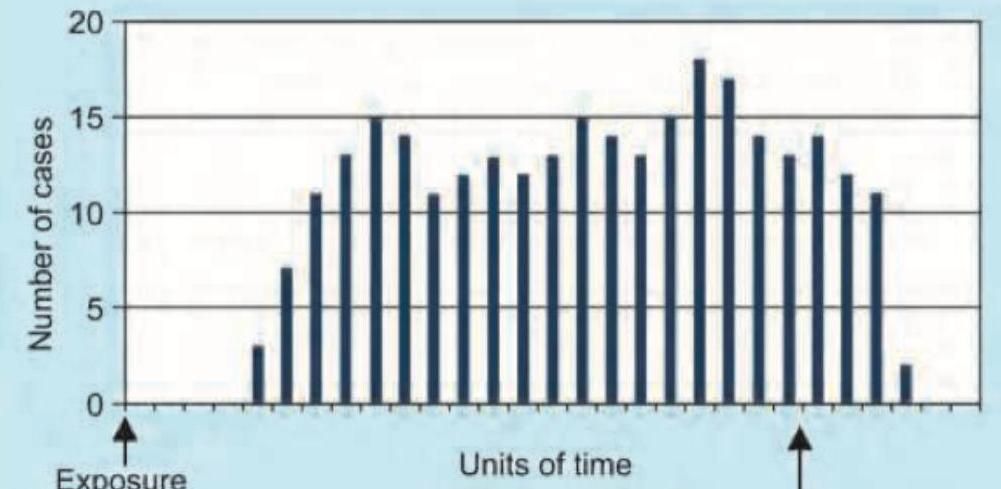
The following diagram shows:
Data obtained from hospital records is not a representative sample of the population. What are the reasons for this ? I. Mild cases and subclinical cases may be missed. II. Population served by a hospital usually cannot be defined. III. Cost of hospital care is not recorded. IV. Admission policy for cases can vary from hospital to hospital. Select the correct answer using the code given below :
John Snow's discovery that cholera is a waterborne disease was the outcome of which type of study?
Many patients with unexplained rash and fever were reported from a village close to the Primary Health Centre (PHC). What is the first step in initiating the investigation of such an epidemic?
Which one of the following terms is an "all-or-none phenomenon" and is best described as termination of all transmission of infection by extermination of the infectious agent?
Which of the following are criteria for cancer screening? I. Screening test should be sensitive and specific II. Screening test should be acceptable to the screened population III. The disease should be an uncommon one for screening to be effective IV. Disease should be recognisable at an early stage Select the correct answer using the code given below :
In which one of the following diseases are the source of infection and reservoir of infection the same ?
The Sample Registration System (SRS), an important source of health information consists of continuous enumeration of births and deaths by an enumerator and an independent survey every six months by an investigator-supervisor. Which one of the following terms best describes this system ?
Practice by Chapter
Principles of Epidemiology
Practice Questions
Measures of Disease Frequency
Practice Questions
Epidemiological Study Designs
Practice Questions
Descriptive Epidemiology
Practice Questions
Analytical Epidemiology
Practice Questions
Experimental Epidemiology
Practice Questions
Screening for Disease
Practice Questions
Surveillance Systems
Practice Questions
Investigation of an Epidemic
Practice Questions
Association and Causation
Practice Questions
Modern Epidemiological Methods
Practice Questions
Critical Appraisal of Epidemiological Studies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app