
Epidemiology — MCQs

On this page
A study was conducted to compare MMR vaccine history in children with autism and children without autism. What kind of study is being done here?
Alleles of a gene pool belong to a:
During the Maha Kumbh Mela, mobile health units were established along with multiple surveillance units. The syndromic surveillance was done based on symptoms like fever and diarrhea. The main purpose of this surveillance is:
In the "De facto" method of census data collection, information is collected based on which of the following?
In a district-level survey, the introduction of breast cancer screening showed an increased 5-year survival rate, but autopsy data revealed no change in mortality. What type of bias does this represent?
A diabetic patient with COVID-19 dies in the hospital. Which type of surveillance does this death report fall under?
Identify the scientist shown in the image below:
The scientist shown in the image below conducted a landmark 1747 experiment aboard naval vessels, dividing scurvy-afflicted sailors into groups and demonstrating that citrus fruits could prevent and cure the disease. Who is this scientist?
What does C in the given image denote?
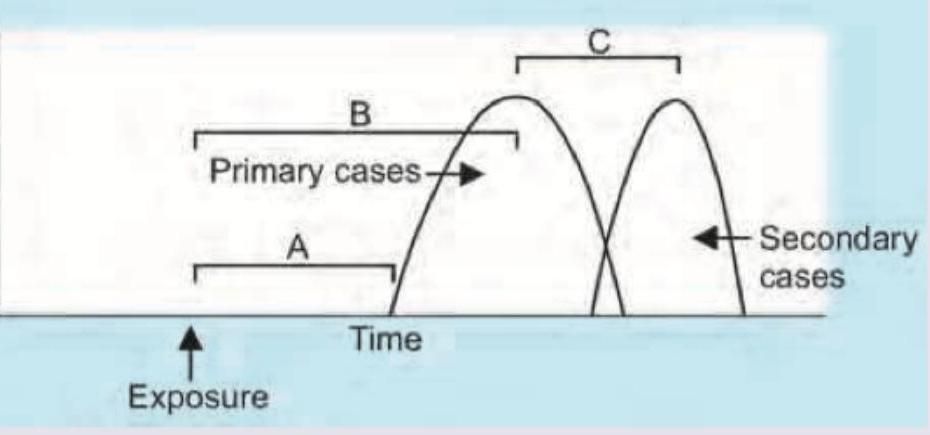
The epidemic curve shown in the image represents which type of outbreak pattern?
Practice by Chapter
Principles of Epidemiology
Practice Questions
Measures of Disease Frequency
Practice Questions
Epidemiological Study Designs
Practice Questions
Descriptive Epidemiology
Practice Questions
Analytical Epidemiology
Practice Questions
Experimental Epidemiology
Practice Questions
Screening for Disease
Practice Questions
Surveillance Systems
Practice Questions
Investigation of an Epidemic
Practice Questions
Association and Causation
Practice Questions
Modern Epidemiological Methods
Practice Questions
Critical Appraisal of Epidemiological Studies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app