
Epidemiology — MCQs

On this page
In a population of 10,000 people, there were 200 deaths in a year. Out of those, 40 died due to HIV. What is the proportional mortality rate from HIV?
Inanimate objects involved in the transmission of infectious agents are considered which of the following?
Which stage of epidemic spread is characterized by a late expanding phase?
In an epidemic of hepatitis E, infection in which of the following carries a poor prognosis?
Prevention of disease by immunization comes under which category of prevention?
All are steps of investigation of an epidemic except?
Which of the following is a live oral vaccine?
The "floating tip of the iceberg" phenomenon in epidemiology represents which of the following?
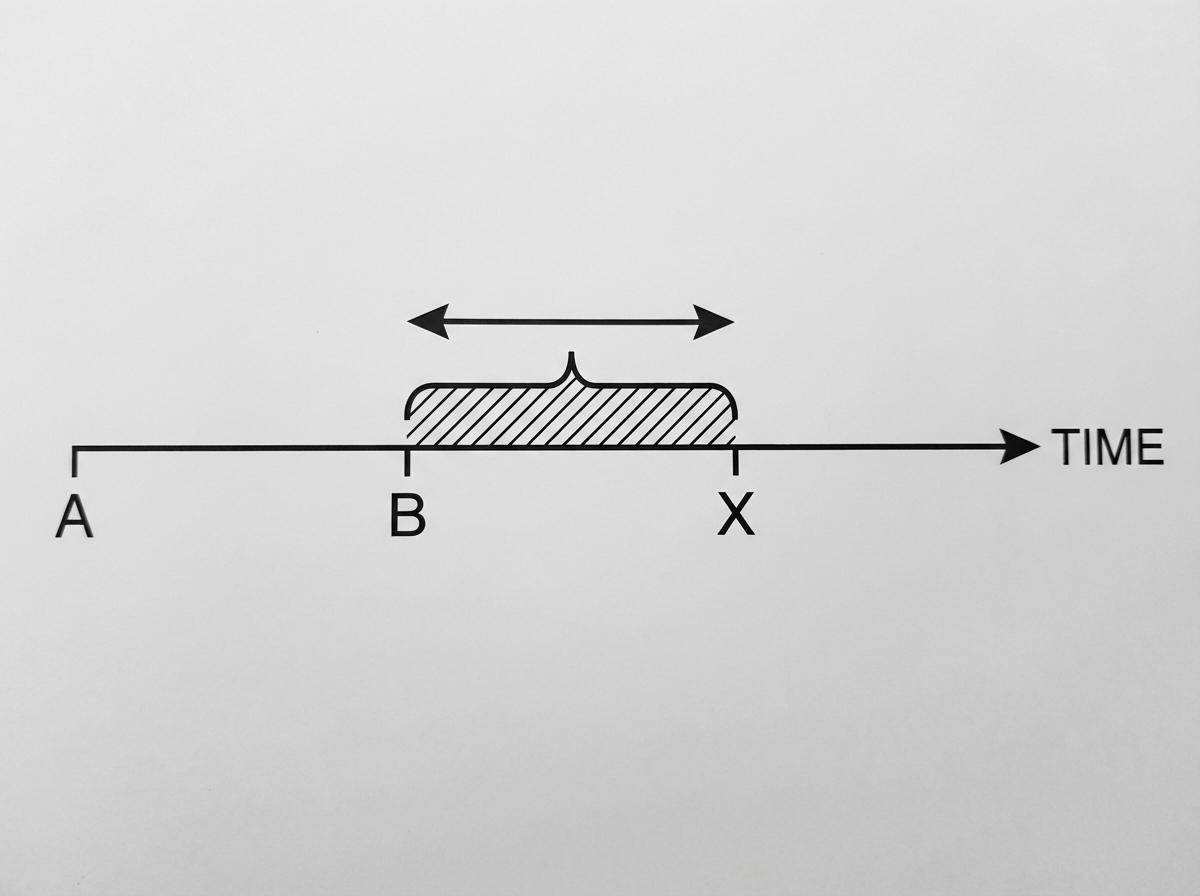
In the natural history of a disease, what does B-X duration represent?
A one-day census of inpatients in a mental hospital could provide what type of information?
Practice by Chapter
Principles of Epidemiology
Practice Questions
Measures of Disease Frequency
Practice Questions
Epidemiological Study Designs
Practice Questions
Descriptive Epidemiology
Practice Questions
Analytical Epidemiology
Practice Questions
Experimental Epidemiology
Practice Questions
Screening for Disease
Practice Questions
Surveillance Systems
Practice Questions
Investigation of an Epidemic
Practice Questions
Association and Causation
Practice Questions
Modern Epidemiological Methods
Practice Questions
Critical Appraisal of Epidemiological Studies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app