
Epidemiology — MCQs

On this page
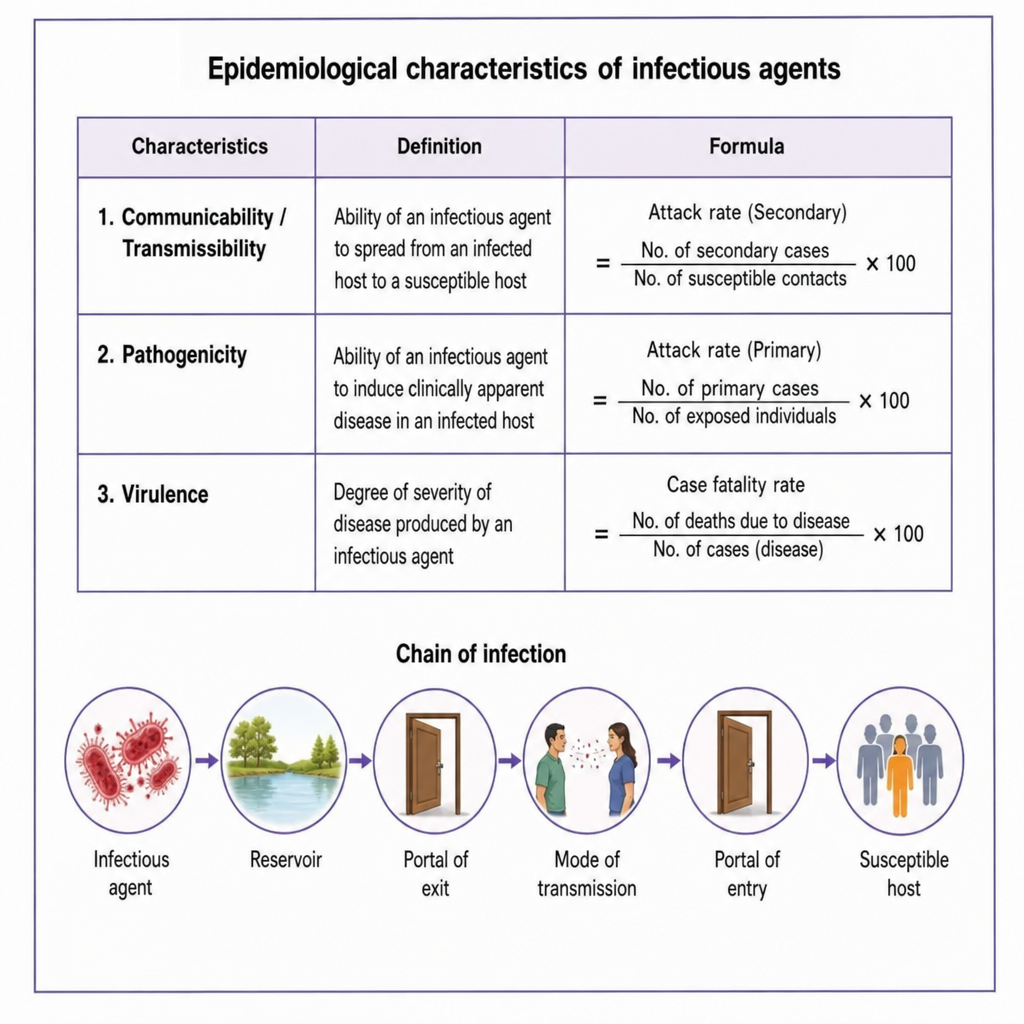
Which of the following epidemiological characteristics are used to measure the ability of biological agents to induce clinically apparent illness?
The window period is defined as the time taken from:
Sullivan's index measures which of the following?
According to the latest WHO classification and measurement of disability, what is the correct terminology?
Point prevalence studies tend to overestimate the occurrence of which of the following diseases?
Which of the following terms best describes the ability of an infectious agent to cause disease?
Which of the following medical events occurred before 1900 AD?
Which of the following is FALSE regarding longitudinal studies?
Which of the following represents the most logical sequence of the progression of a health condition?
Generation time in epidemiology is defined as?
Practice by Chapter
Principles of Epidemiology
Practice Questions
Measures of Disease Frequency
Practice Questions
Epidemiological Study Designs
Practice Questions
Descriptive Epidemiology
Practice Questions
Analytical Epidemiology
Practice Questions
Experimental Epidemiology
Practice Questions
Screening for Disease
Practice Questions
Surveillance Systems
Practice Questions
Investigation of an Epidemic
Practice Questions
Association and Causation
Practice Questions
Modern Epidemiological Methods
Practice Questions
Critical Appraisal of Epidemiological Studies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app