
Epidemiology — MCQs

On this page
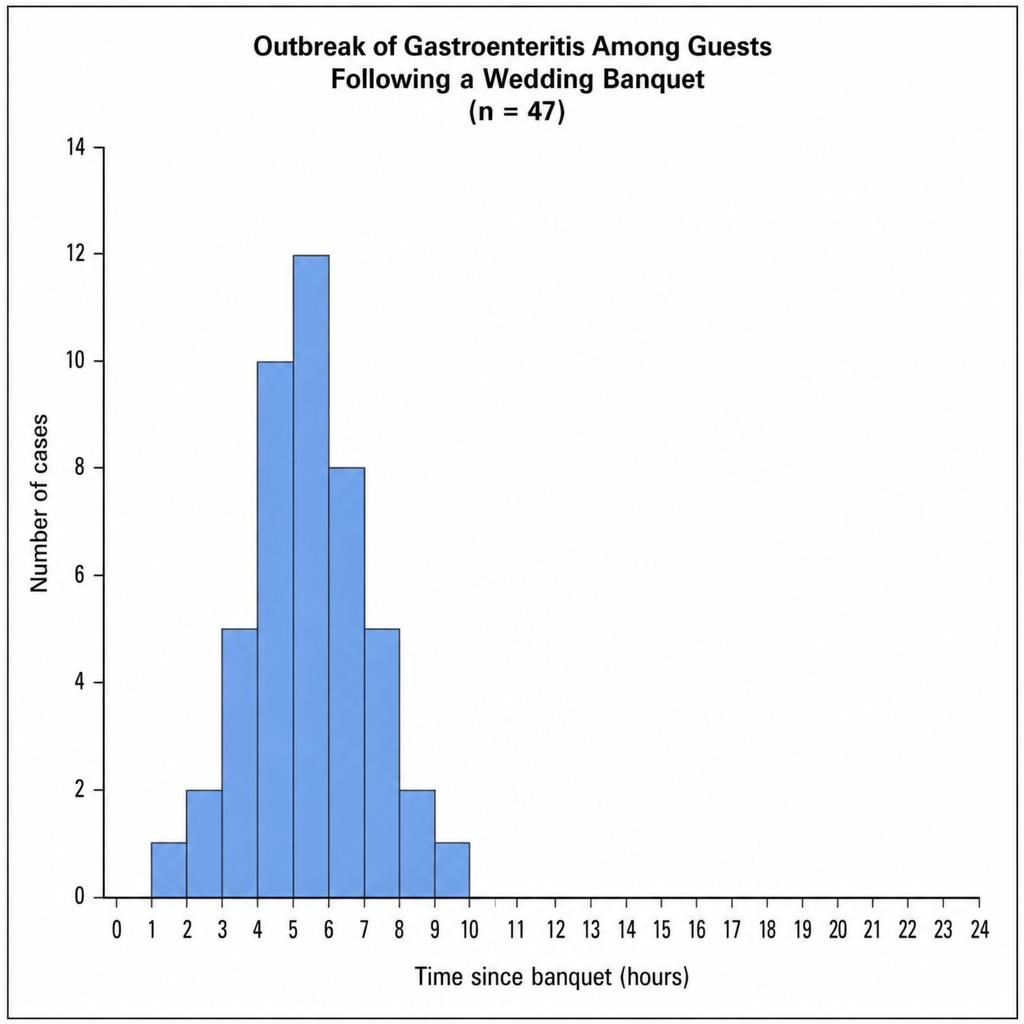
Following a wedding banquet attended by 200 guests in a rural village, the district health officer receives reports of 47 guests developing nausea, vomiting, and diarrhea within hours of the meal. Cases are line-listed and plotted by hour of symptom onset after the banquet. The epi-curve is shown in Image 1. Based on this curve, what is the MOST appropriate immediate public health action?
A novel rapid diagnostic test for visceral leishmaniasis shows sensitivity of 85% and specificity of 90% in controlled trials. When deployed in a region with 2% prevalence of VL (as determined by gold standard testing), public health officials note that most positive results are false positives. Evaluate the most appropriate strategy to improve the program's effectiveness.
A community health analysis shows Region A has higher crude mortality rate than Region B, but age-standardized mortality rate is lower in Region A. What is the most likely explanation?
A novel coronavirus outbreak is detected with high transmissibility but variable mortality across age groups. Phylogenetic analysis shows 80% similarity with SARS-CoV. To predict pandemic potential, which epidemiological parameter would be most critical to evaluate first?
A deep learning algorithm for detecting pneumonia on chest X-rays performs excellently on the validation set but poorly on external testing. Analysis reveals the algorithm learned to recognize the hospital logo and text on images from ICU patients (who more likely had pneumonia). What type of bias does this represent?
Which of the following infectious diseases has the lowest incubation period?
Major epidemics are due to which of the following characteristics of the pathogen?
Which of the following is NOT a measure of morbidity?
Iodised salt is given in an area endemic to goiter. What type of prevention is this?
What is a confounding factor associated with?
Practice by Chapter
Principles of Epidemiology
Practice Questions
Measures of Disease Frequency
Practice Questions
Epidemiological Study Designs
Practice Questions
Descriptive Epidemiology
Practice Questions
Analytical Epidemiology
Practice Questions
Experimental Epidemiology
Practice Questions
Screening for Disease
Practice Questions
Surveillance Systems
Practice Questions
Investigation of an Epidemic
Practice Questions
Association and Causation
Practice Questions
Modern Epidemiological Methods
Practice Questions
Critical Appraisal of Epidemiological Studies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app