
Epidemiology — MCQs

On this page
Consider the following vectors: 1. Aedes mosquito 2. Flea 3. Ticks 4. Itchmite Transovarian transmission is demonstrated in
Consider the following diseases: 1. Rift valley fever 2. Yellow Fever 3. Chikungunya fever 4. West Nile fever Which of the above diseases are transmitted by Aedes mosquito?
The time period from entry of an infective agent into a host until the host develops the capacity for maximal infectivity is called:
A village 'X' has a population of 5000 with a birth rate of 25 per thousand. In any given month, how many pregnancies should be registered with the ANM of this village?
Association between hardness of drinking water and death rate from cardiovascular diseases is:
Which one of the following epidemiologic methods can be used to identify risk factors and estimate the degree of risk?
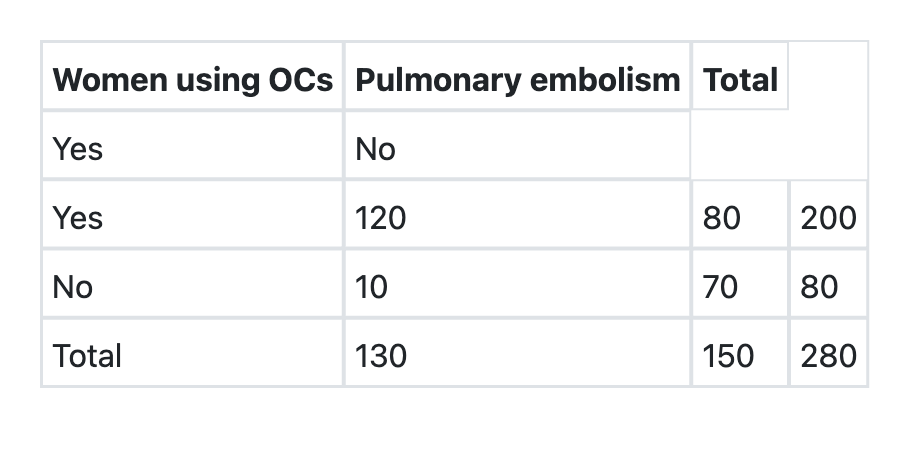
What is the relative risk of developing pulmonary embolism in users of oral contraceptives as per the information given below?
In a family of six (2 parents and 4 children), the youngest child catches measles infection. The parents are immune to the infection. On 3rd and 5th day of the infection of the first child, the two other children also suffer from measles. The secondary attack rate (SAR) of measles is:
Standardized Mortality ratio is best explained by which one of the following statements?
In a case-control study, 300 women aged 20-45 years suffering from breast cancer were compared with age-matched 300 women without breast cancer. It was observed that 120 women among cases and 60 women among controls were obese. The odds ratio of developing breast cancer among obese women is:
Practice by Chapter
Principles of Epidemiology
Practice Questions
Measures of Disease Frequency
Practice Questions
Epidemiological Study Designs
Practice Questions
Descriptive Epidemiology
Practice Questions
Analytical Epidemiology
Practice Questions
Experimental Epidemiology
Practice Questions
Screening for Disease
Practice Questions
Surveillance Systems
Practice Questions
Investigation of an Epidemic
Practice Questions
Association and Causation
Practice Questions
Modern Epidemiological Methods
Practice Questions
Critical Appraisal of Epidemiological Studies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app