
Epidemiology — MCQs

On this page
Which one of the following experiments/trials is a part of non-randomized trials?
A well of contaminated water resulted in an outbreak of diarrhoea in a community. Which type of epidemic will this exposure present with? 1.Propagated epidemic 2.Common source - continuous exposure 3.Common source - point exposure
The yield of a screening test CAN NOT be increased by which of the following?
What are the characteristics of ideal health indicators?
After attending a birthday party in a hostel around 50 students reported having loose stools, fever and a few reported vomiting. This outbreak can be identified as what type of outbreak ?
In a town with one lakh population (1,00,000) there are a total of 2500 live births in a year. There were 75 total deaths of children before the age of one month, total 200 deaths before the age of one year, and a total 300 deaths before the age of three years. Which of the following statements regarding Infant Mortality Rate (IMR) of the town for the given year are correct? 1. The denominator is 1,00,000 2. The IMR of the town is higher than the current national average of IMR for India 3. The numerator is the number of children dying before the age of one month 4. The IMR of the town is 80 per 1000 live births
Which one of the following is a famous large prospective study that helped establish risk factors for coronary heart disease ?
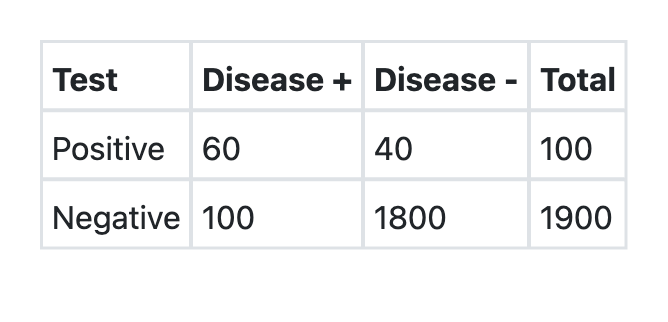
A new test was developed for detection of COVID-19. What is the sensitivity of the test as per the information provided above?
Which one of the following best explains the relationship among Prevalence (P), Incidence (I) and Duration (D) of a disease given the assumption that the population is stable ?
In which one of the following study designs, the unit of study involves populations rather than individuals ?
Practice by Chapter
Principles of Epidemiology
Practice Questions
Measures of Disease Frequency
Practice Questions
Epidemiological Study Designs
Practice Questions
Descriptive Epidemiology
Practice Questions
Analytical Epidemiology
Practice Questions
Experimental Epidemiology
Practice Questions
Screening for Disease
Practice Questions
Surveillance Systems
Practice Questions
Investigation of an Epidemic
Practice Questions
Association and Causation
Practice Questions
Modern Epidemiological Methods
Practice Questions
Critical Appraisal of Epidemiological Studies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app