
Epidemiology — MCQs

On this page
Chandler’s index is used in the epidemiological studies of
When the prevalence rate is used without any qualification, it is taken to mean as
Which of the following Screening methods for Disease is the least useful?
By which one of the following studies can relative risk be best calculated?
Which of the following is/are suggested by rising incidence rates of any disease? 1. Need for a new disease control programme 2. Improvement in reporting practices 3. Change in the etiology of the disease Select the correct answer using the codes given below:
Which of the following types of study designs will be most appropriate to find out the association between mobile phone radiation exposure and cancer?
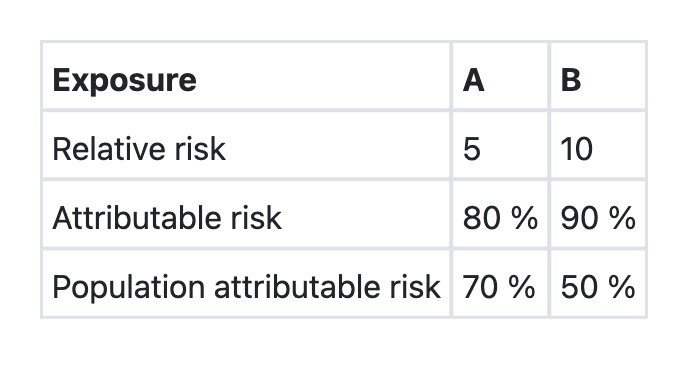
The data regarding two exposures A and B, associated with a disease X in a community is given below: Which one of the following assertions and the reasons given is correct?
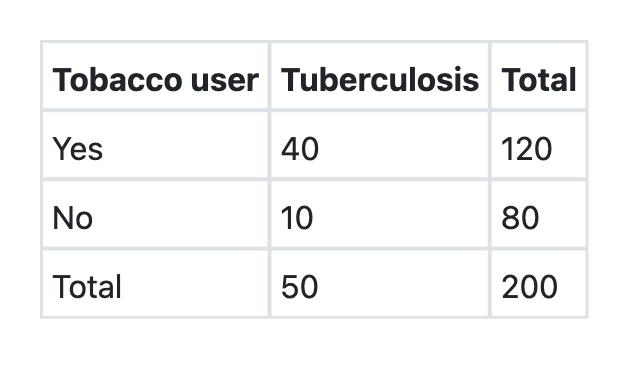
A cohort study was conducted among 200 men aged 20–30 years in Rampur village. Out of 200, 120 men were tobacco users and rest 80 didn’t take any form of tobacco. At the end of one year, 40 men among tobacco users and 10 men among non-tobacco users developed tuberculosis. The incidence of tuberculosis among tobacco users is:
What is the attributable risk percent (etiologic fraction) of tobacco for developing tuberculosis as per the information given below? Tobacco users Tuberculosis Total Present Absent Yes 40 80 120 No 10 70 80 Total 50 150 200
What is the relative risk of developing tuberculosis among tobacco users as per the information given below?
Practice by Chapter
Principles of Epidemiology
Practice Questions
Measures of Disease Frequency
Practice Questions
Epidemiological Study Designs
Practice Questions
Descriptive Epidemiology
Practice Questions
Analytical Epidemiology
Practice Questions
Experimental Epidemiology
Practice Questions
Screening for Disease
Practice Questions
Surveillance Systems
Practice Questions
Investigation of an Epidemic
Practice Questions
Association and Causation
Practice Questions
Modern Epidemiological Methods
Practice Questions
Critical Appraisal of Epidemiological Studies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app