
Epidemiology — MCQs

On this page
Which among the following countries is a 'Rabies free country'?
Pearl's index indicates:
Which of the following terms denotes the approximate magnitude of completed family size?
What is the definition of an index case?
The 'dependency ratio' includes age groups that are:
What is the secondary attack rate of pertussis in unimmunized household contacts of a pertussis case?
What is a case-control study?
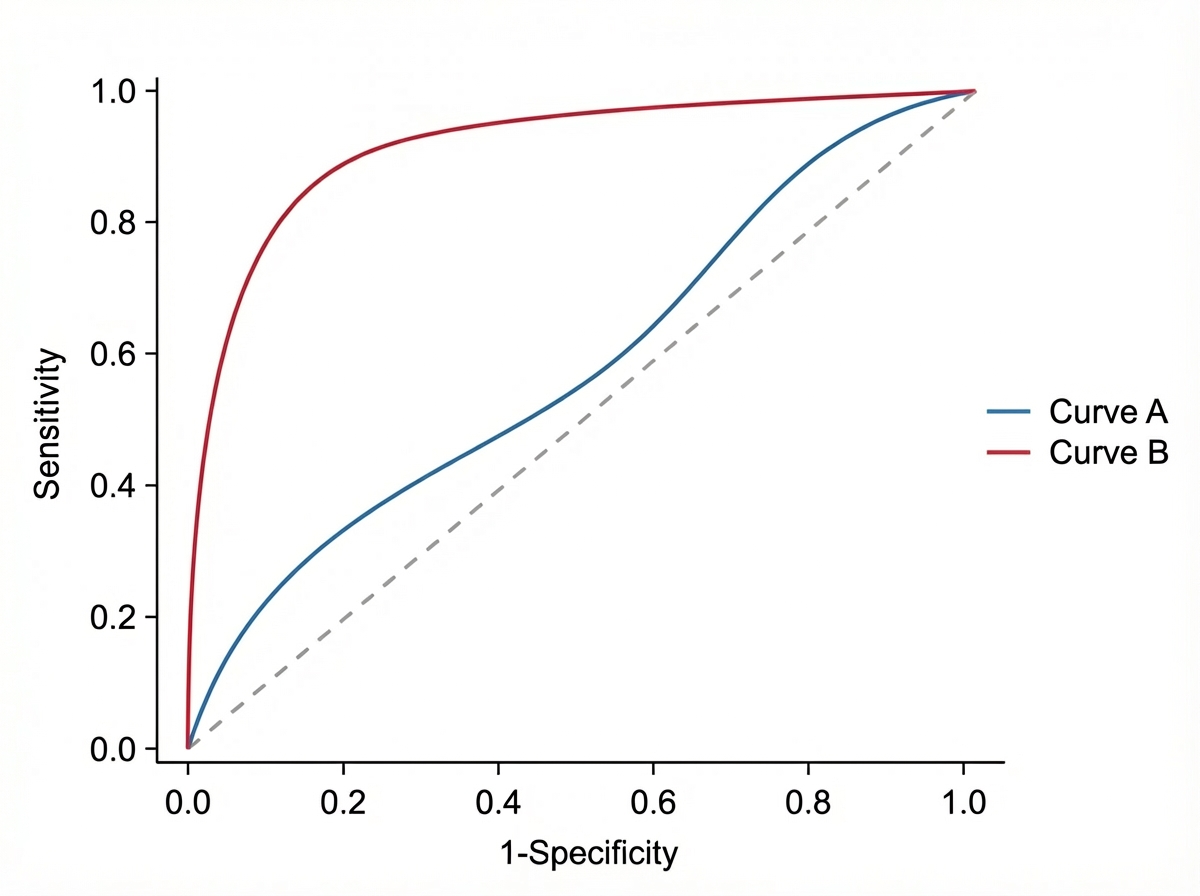
Observe the following curves. What will happen to Sensitivity and Specificity if the curve changes from Blue to Red?
What is the primary level of prevention?
The prevalence of a disease depends upon which of the following factors?
Practice by Chapter
Principles of Epidemiology
Practice Questions
Measures of Disease Frequency
Practice Questions
Epidemiological Study Designs
Practice Questions
Descriptive Epidemiology
Practice Questions
Analytical Epidemiology
Practice Questions
Experimental Epidemiology
Practice Questions
Screening for Disease
Practice Questions
Surveillance Systems
Practice Questions
Investigation of an Epidemic
Practice Questions
Association and Causation
Practice Questions
Modern Epidemiological Methods
Practice Questions
Critical Appraisal of Epidemiological Studies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app