
Epidemiology — MCQs

On this page
A suspected cause preceding an observed effect is an example of which criterion for causality?
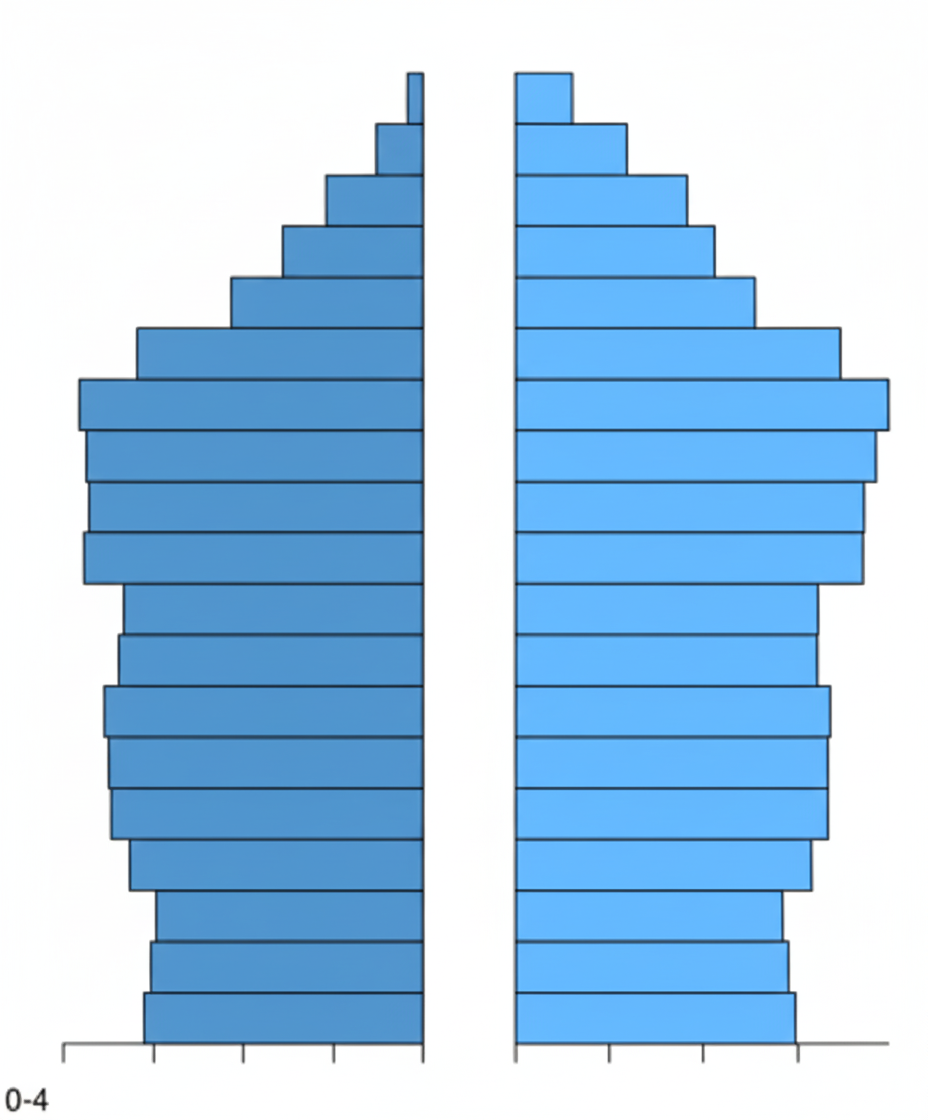
Which type of age pyramid is shown in the image?
If two screening tests are used in parallel, what is the effect on their predictive values?
What will be the Odds Ratio if diseased with risk factor = a; diseased without risk factor = b; not diseased but with risk factor = c; and not diseased as well as not with risk factor = d?
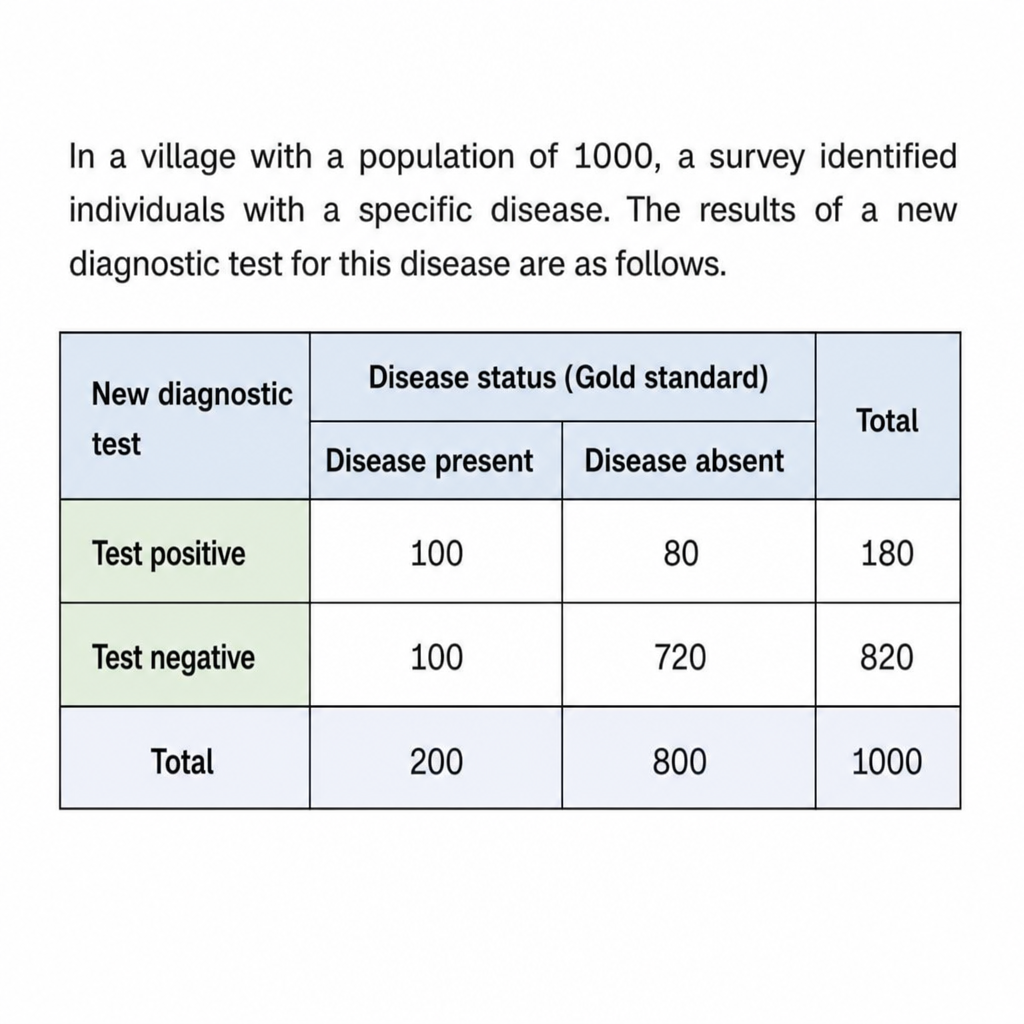
In a village with a population of 1000, a survey identified individuals with a specific disease. The results of a new diagnostic test for this disease are as follows. What is the percentage prevalence of the disease?
If 25 persons are working on a project for 30 years, how many person-years of employment are there?
Which of the following conditions is characterized by an incubatory carrier state?
A couple has 4 unvaccinated children for measles. One child contracted measles on August 5th, 2015, and two other children developed measles by August 15th, 2015. What is the secondary attack rate in this scenario?
Mandatory washing of hands by a physician after examining each patient can reduce the incidence of iatrogenic infections. This is an example of:
Which of the following rates is an indicator of both mortality and the living standard of a community?
Practice by Chapter
Principles of Epidemiology
Practice Questions
Measures of Disease Frequency
Practice Questions
Epidemiological Study Designs
Practice Questions
Descriptive Epidemiology
Practice Questions
Analytical Epidemiology
Practice Questions
Experimental Epidemiology
Practice Questions
Screening for Disease
Practice Questions
Surveillance Systems
Practice Questions
Investigation of an Epidemic
Practice Questions
Association and Causation
Practice Questions
Modern Epidemiological Methods
Practice Questions
Critical Appraisal of Epidemiological Studies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app