
Molecular Biology and Genomics — MCQs

On this page
Recombinant human insulin is made by -
DNA fingerprinting was discovered by:
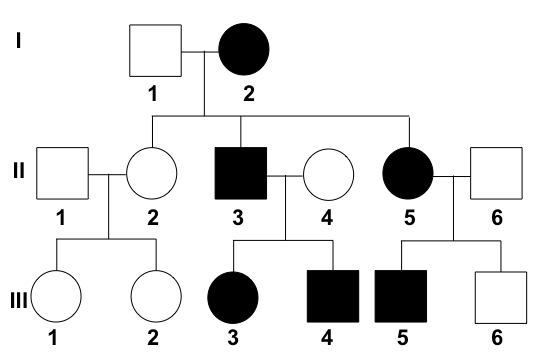
Examine this pedigree chart carefully. What type of transmission does it depict?
The term restriction map primarily refers to the mapping of sites of
Apolipoprotein B-48 is made by which process?
Mark the false statement regarding mitochondrial DNA:
Klenow fragment is formed by loss of fragment having which activity?
In CRISPR-Cas9 system, which repair mechanism is predominantly used for genome editing?
Which of the following doesn't occur in 5' to 3' direction?
Which of the following binds mRNA with ribosome in prokaryotes?
Practice by Chapter
DNA Replication and Repair Mechanisms
Practice Questions
Transcription Factors and Gene Regulation
Practice Questions
Epigenetics and DNA Methylation
Practice Questions
RNA Processing and Splicing
Practice Questions
miRNA and RNA Interference
Practice Questions
Protein Synthesis and Post-Translational Modifications
Practice Questions
Genomics and Human Genome Project
Practice Questions
Single Nucleotide Polymorphisms
Practice Questions
Gene Therapy Approaches
Practice Questions
CRISPR-Cas9 and Genome Editing
Practice Questions
DNA Fingerprinting and Forensics
Practice Questions
Molecular Basis of Genetic Diseases
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app