
Carbohydrate Metabolism — MCQs

On this page
A 30-year-old patient presents with intractable vomiting and inability to eat or drink for the past 3 days. Their blood glucose level remains normal. Which of the following is most important for the maintenance of blood glucose in this patient?
Glucuronic acid and Iduronic acid are:
McArdle's disease is due to deficiency of which enzyme?
A female infant appeared normal at birth but developed signs of liver disease and muscular weakness at 3 months. She had periods of hypoglycemia, particularly on awakening. Examination revealed hepatomegaly. Laboratory analyses following fasting revealed ketoacidosis, blood pH 7.25, and elevations in both alanine transaminase (ALT) and aspartate transaminase (AST). Administration of glucagon following a carbohydrate meal elicited a normal rise in blood glucose, but glucose levels did not rise when glucagon was administered following an overnight fast. Liver biopsy revealed an increase in the glycogen content. To prevent the frequent episodes of hypoglycemia, which of the following dietary supplements would be most appropriate for this patient?
Which of the following carbohydrates is not digested in humans?
A 6-month-old infant presents with bilateral cataracts. What metabolic disorder should be suspected if a urine test is performed?
A 7-month-old infant, recently started on top feeds, presented with diarrhea, vomiting, nausea, abdominal pain, and distension, leading to poor feeding and poor weight gain. On examination, hepatosplenomegaly was observed. Lab findings include decreased blood sugar, increased serum bilirubin, and increased uric acid. A reducing substance was found in the urine during the episode of hypoglycemia. Which of the following statements is FALSE about this condition?
Cloudy cornea is a feature of which of the following diseases?
Glucagon will decrease which of the following?
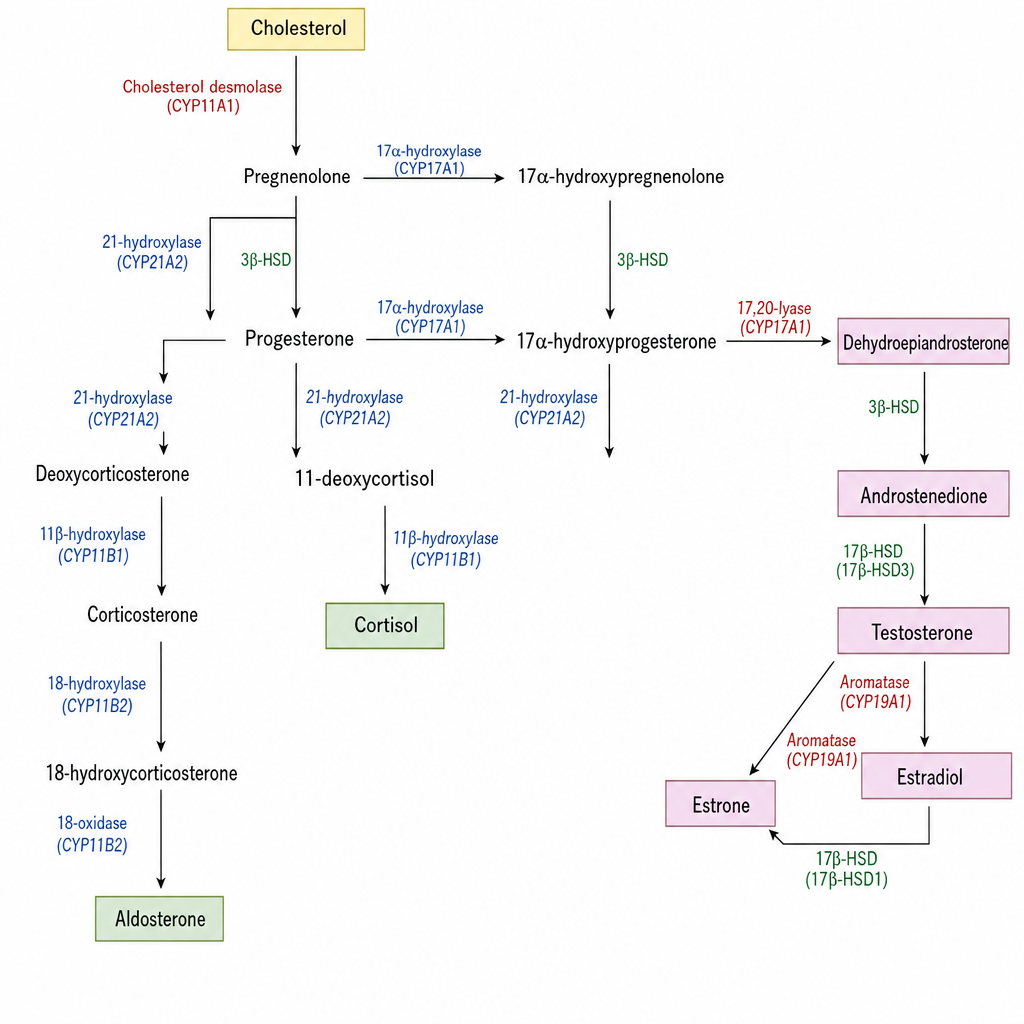
The figure depicts the steroidogenesis pathway. The corticosteroid-producing branches of this pathway are seen in which of the following organ(s)?
Practice by Chapter
Carbohydrate Chemistry and Classification
Practice Questions
Glycolysis: Reactions and Regulation
Practice Questions
Gluconeogenesis: Reactions and Regulation
Practice Questions
Glycogen Metabolism: Synthesis and Breakdown
Practice Questions
Glycogen Storage Diseases
Practice Questions
Pentose Phosphate Pathway
Practice Questions
Metabolism of Fructose and Galactose
Practice Questions
Disorders of Fructose and Galactose Metabolism
Practice Questions
Blood Glucose Regulation
Practice Questions
Diabetes Mellitus: Biochemical Aspects
Practice Questions
Glycosylation and Glycoproteins
Practice Questions
Lactose Intolerance and Galactosemia
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app