
Carbohydrate Metabolism — MCQs

On this page
Which of the following cell pathways occurs exclusively in cell cytoplasm?
Cancer cells take up excess glucose because?
A child presents with fatigue and hepatomegaly. Liver enzymes (ALT, AST) are elevated. Ketosis was significant. Liver biopsy shows excess glycogen accumulation. After feeding, blood glucose levels rise, but there is no rise in glucose after overnight fasting. Which of the following enzyme deficiencies is most likely responsible for this presentation?
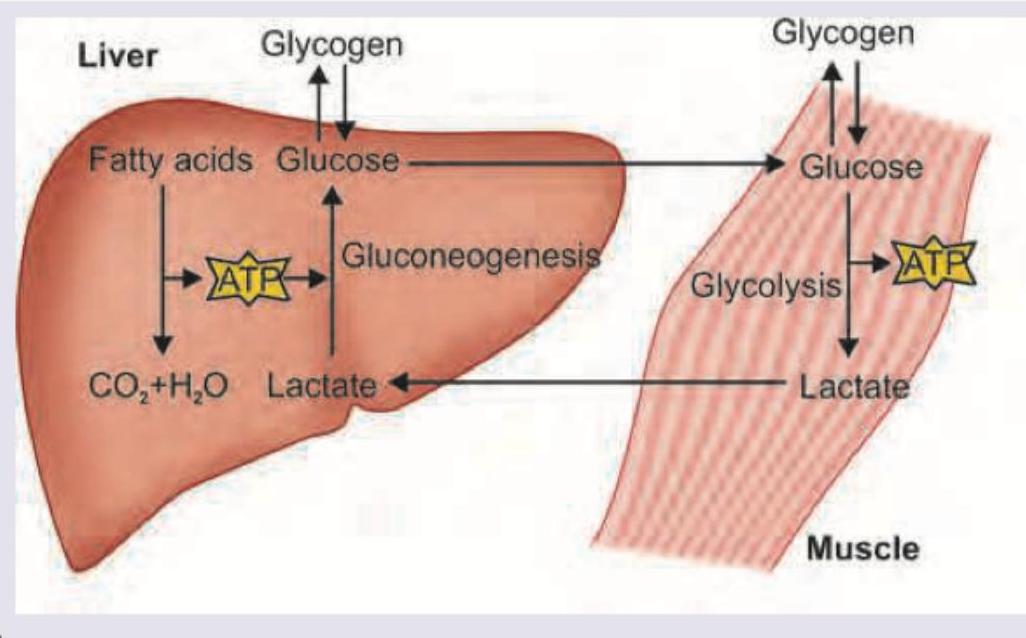
What is the cycle shown below called?
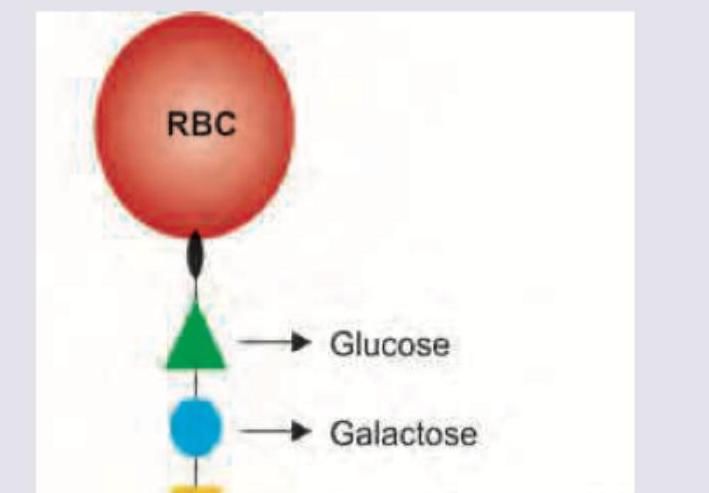
Name the antigen marked as X determining blood group A.
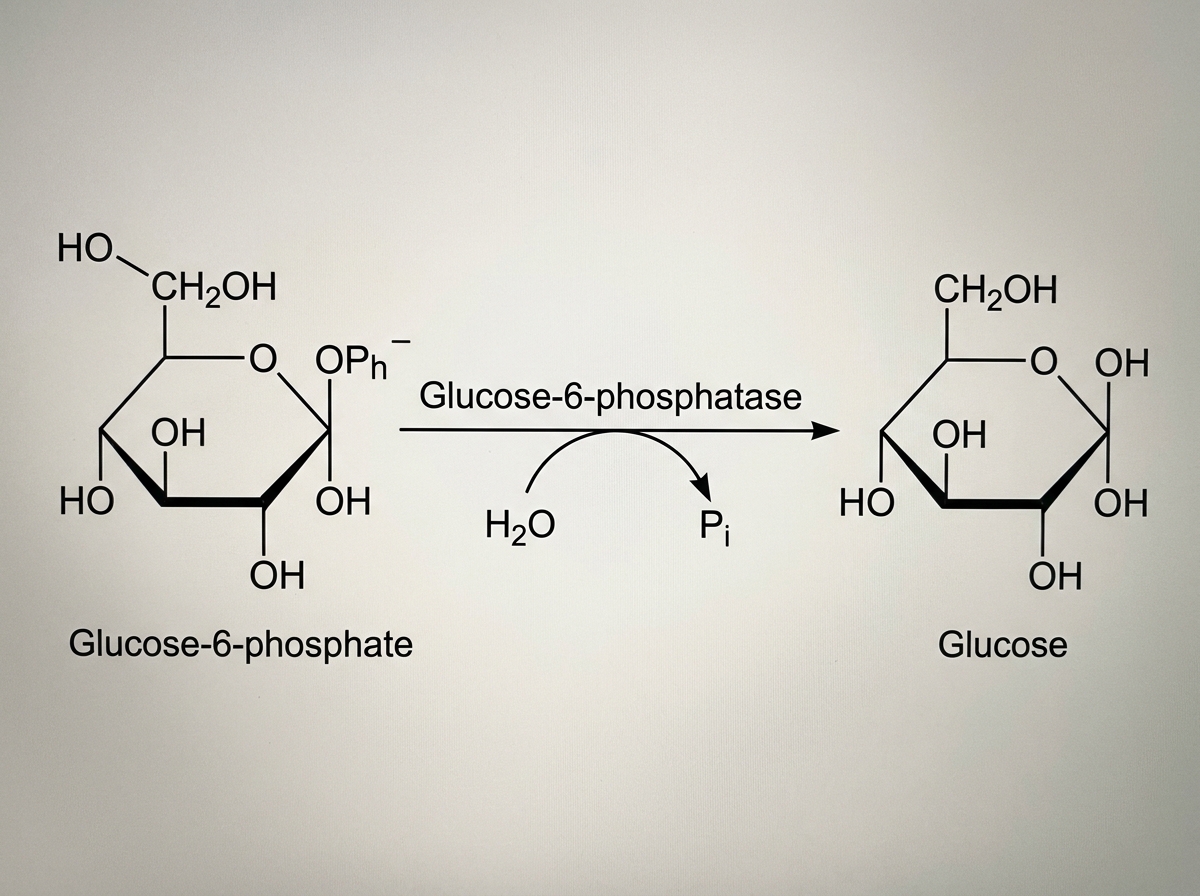
The enzyme catalyzing this pathway is absent in?
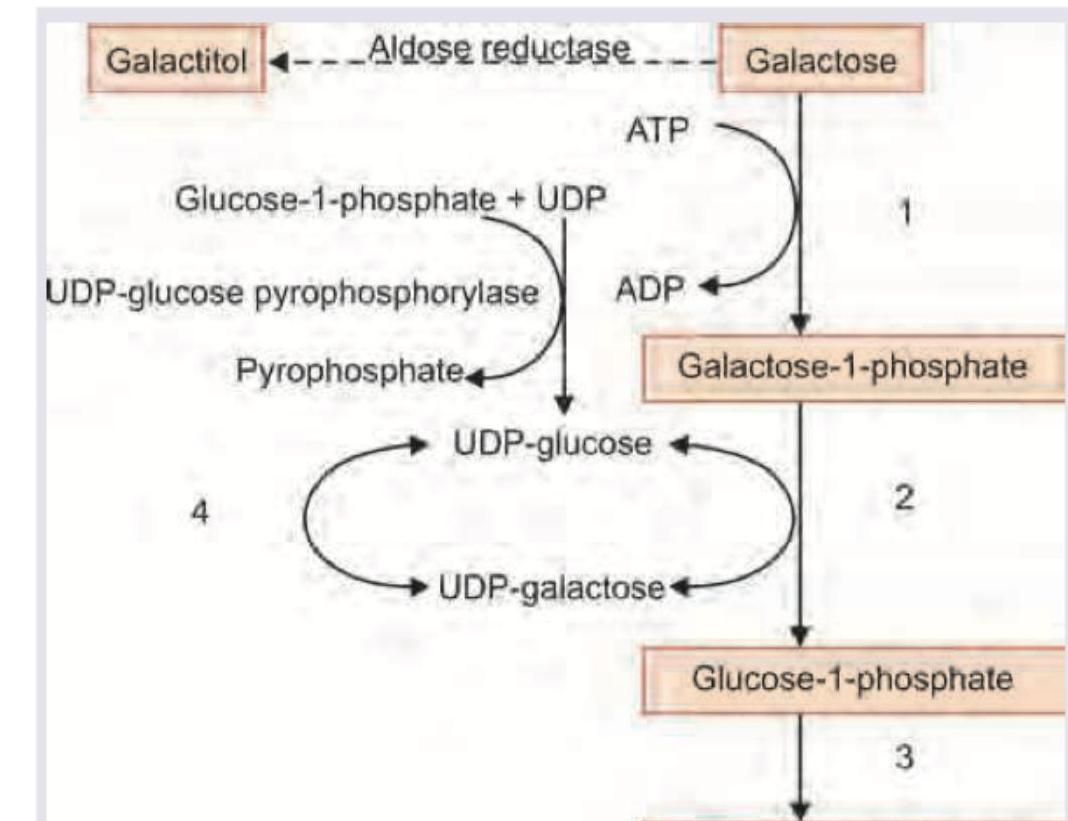
A 2-week-old neonate is brought with complaints of recurrent vomiting, prolongation of physiological jaundice. Urine tests negative for sugar by dipstick but Benedict's test is positive. Which of the following enzymatic defect is most likely responsible for this presentation?
A floppy infant was brought with difficulty in breathing. CXR was performed. Family history was positive for death of sibling at 1-year of age. Which of the following enzyme deficiency will lead to this presentation?
Which transporter helps in the improvement of insulin resistance in type 2 diabetes mellitus (DM2) with regular exercise and physical activities?
Corneal Transparency is maintained by which of the following GAGs?
Practice by Chapter
Carbohydrate Chemistry and Classification
Practice Questions
Glycolysis: Reactions and Regulation
Practice Questions
Gluconeogenesis: Reactions and Regulation
Practice Questions
Glycogen Metabolism: Synthesis and Breakdown
Practice Questions
Glycogen Storage Diseases
Practice Questions
Pentose Phosphate Pathway
Practice Questions
Metabolism of Fructose and Galactose
Practice Questions
Disorders of Fructose and Galactose Metabolism
Practice Questions
Blood Glucose Regulation
Practice Questions
Diabetes Mellitus: Biochemical Aspects
Practice Questions
Glycosylation and Glycoproteins
Practice Questions
Lactose Intolerance and Galactosemia
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app