
Carbohydrate Metabolism — MCQs

On this page
In which of the following tissues is glycogen incapable of contributing directly to blood glucose?
Which enzyme is responsible for the complete oxidation of glucose to CO2 and water?
Skeletal muscle is deficient in which of the following enzymes?
Which of the following reactions in the TCA cycle is an example of substrate-level phosphorylation?
A pregnant woman with lactase deficiency cannot tolerate milk in her diet and is concerned about producing milk of insufficient caloric value to nourish her baby. What is the best advice to give her?
The polyol pathway is responsible for the formation of which of the following?
Diabetes mellitus is associated with which type of lactic acidosis?
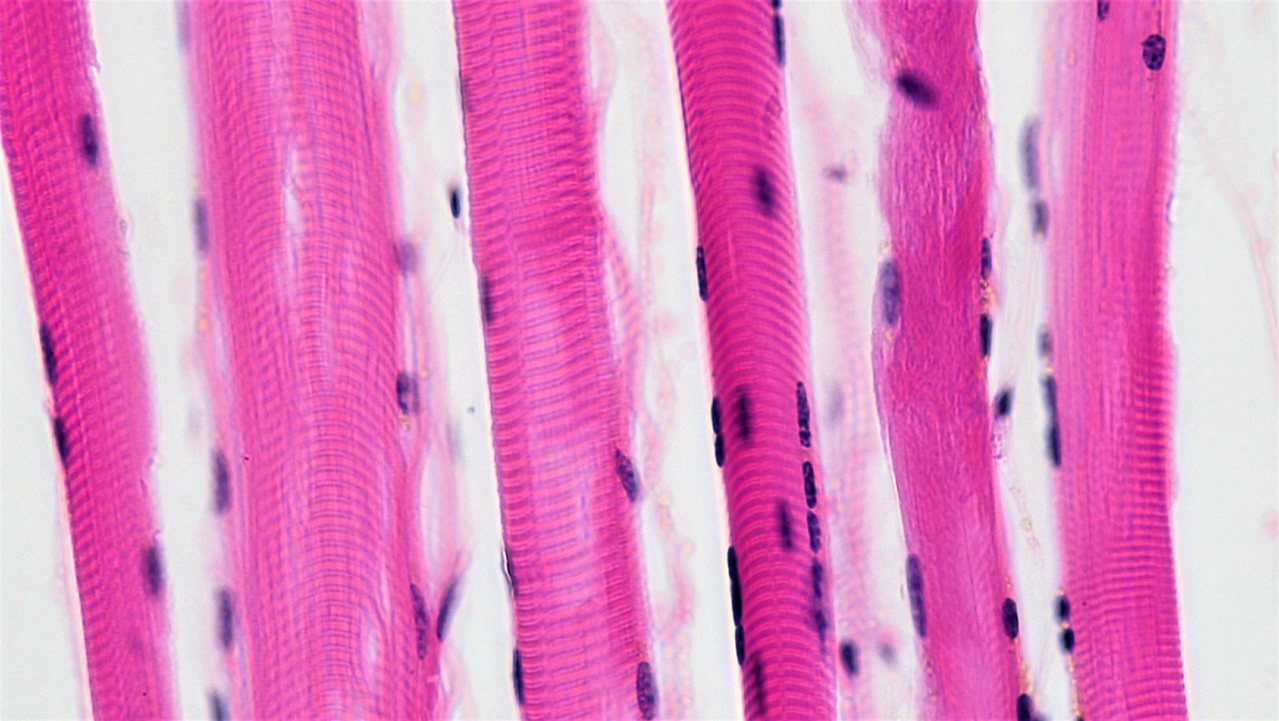
The muscle shown in the illustration predominantly uses which glucose transporter?
Which molecule, known to initiate cataract formation in the eye lens, also has a 1-phosphate derivative responsible for liver failure?
Hers disease is due to deficiency of which enzyme?
Practice by Chapter
Carbohydrate Chemistry and Classification
Practice Questions
Glycolysis: Reactions and Regulation
Practice Questions
Gluconeogenesis: Reactions and Regulation
Practice Questions
Glycogen Metabolism: Synthesis and Breakdown
Practice Questions
Glycogen Storage Diseases
Practice Questions
Pentose Phosphate Pathway
Practice Questions
Metabolism of Fructose and Galactose
Practice Questions
Disorders of Fructose and Galactose Metabolism
Practice Questions
Blood Glucose Regulation
Practice Questions
Diabetes Mellitus: Biochemical Aspects
Practice Questions
Glycosylation and Glycoproteins
Practice Questions
Lactose Intolerance and Galactosemia
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app