
Carbohydrate Metabolism — MCQs

On this page
Which of the following is a reversible enzyme?
G6PD helps in maintaining the integrity of RBC by:
A hypotonic baby shows an increased ratio of Pyruvate to Acetyl CoA. The baby also exhibits features of lactic acidosis. The underlying defect prevents pyruvate from forming Acetyl CoA in fibroblasts. Which of the following can revert this situation?
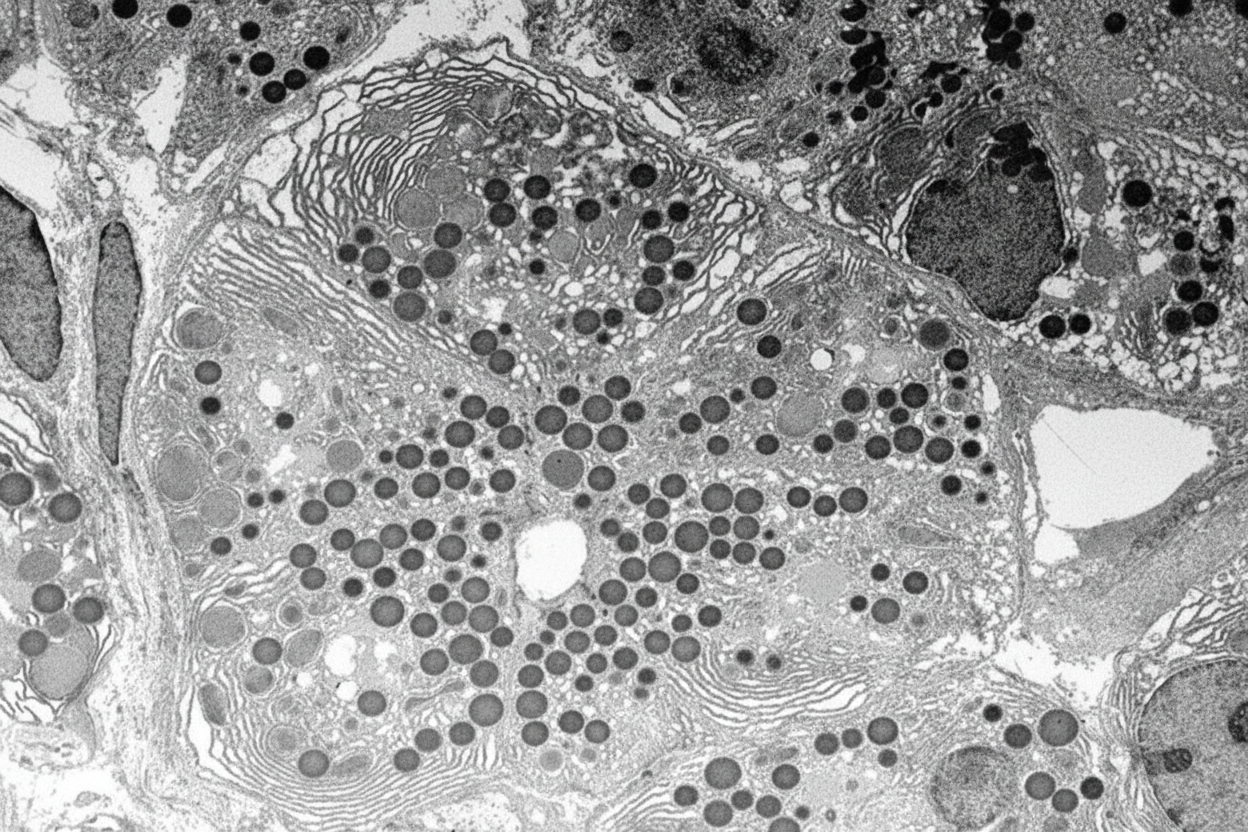
Which of the following enzymes is associated with the ER membrane shown in the given image?
Which of the following is NOT a product of the Hexose Monophosphate (HMP) shunt?
Which of the following is NOT used in gluconeogenesis?
Which of the following glucose transporters is primarily utilized by adipocytes?
What are the enzymes required for the formation of Phosphoenolpyruvate from Pyruvate?
All of the following are true about changes in brain metabolism after traumatic brain injury, except:
Which of the following enzymes becomes deficient following an episode of severe infectious gastroenteritis?
Practice by Chapter
Carbohydrate Chemistry and Classification
Practice Questions
Glycolysis: Reactions and Regulation
Practice Questions
Gluconeogenesis: Reactions and Regulation
Practice Questions
Glycogen Metabolism: Synthesis and Breakdown
Practice Questions
Glycogen Storage Diseases
Practice Questions
Pentose Phosphate Pathway
Practice Questions
Metabolism of Fructose and Galactose
Practice Questions
Disorders of Fructose and Galactose Metabolism
Practice Questions
Blood Glucose Regulation
Practice Questions
Diabetes Mellitus: Biochemical Aspects
Practice Questions
Glycosylation and Glycoproteins
Practice Questions
Lactose Intolerance and Galactosemia
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app