
Regional Anesthesia — MCQs

On this page
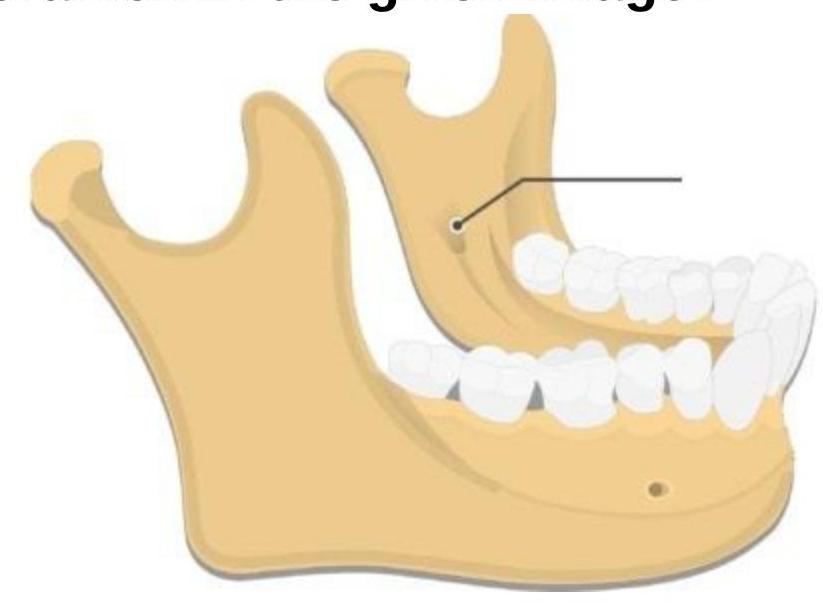
The block shown in the diagram is going to affect all of the following nerves EXCEPT?
Complications of stellate ganglion block include all of the following except?
Differential blockade is achieved by central neuraxial blockade. What is the primary mechanism?
Which of the following is NOT a complication of epidural opioid administration?
Which of the following is FALSE regarding lumbar puncture in patients on anticoagulants or antiplatelets?
Pneumothorax is a known complication of which of the following procedures?
Which drug is contraindicated for Bier's block?
In the extraoral technique for mandibular nerve block, after contacting the pterygoid plate, in which direction is the needle directed?
Which cranial nerve is most commonly involved in spinal anesthesia?
What is the extra-oral landmark for the Gowgates technique of mandibular nerve block?
Practice by Chapter
Neuraxial Anatomy
Practice Questions
Spinal Anesthesia
Practice Questions
Epidural Anesthesia
Practice Questions
Combined Spinal-Epidural Anesthesia
Practice Questions
Peripheral Nerve Blocks: Upper Extremity
Practice Questions
Peripheral Nerve Blocks: Lower Extremity
Practice Questions
Truncal Blocks
Practice Questions
Ultrasound-Guided Regional Anesthesia
Practice Questions
Complications of Regional Anesthesia
Practice Questions
Regional Anesthesia in Pediatric Patients
Practice Questions
Regional Anesthesia in Obstetrics
Practice Questions
Continuous Peripheral Nerve Catheters
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app