
Regional Anesthesia — MCQs

On this page
A patient is placed in the **lateral decubitus position** (lying on their side with knees drawn toward the chest and the spine flexed/arched outward) before the procedure. This position is maintained during which of the following types of anaesthesia?
Identify the instrument shown in the figure below.

Contraindications to epidural analgesia include the following except
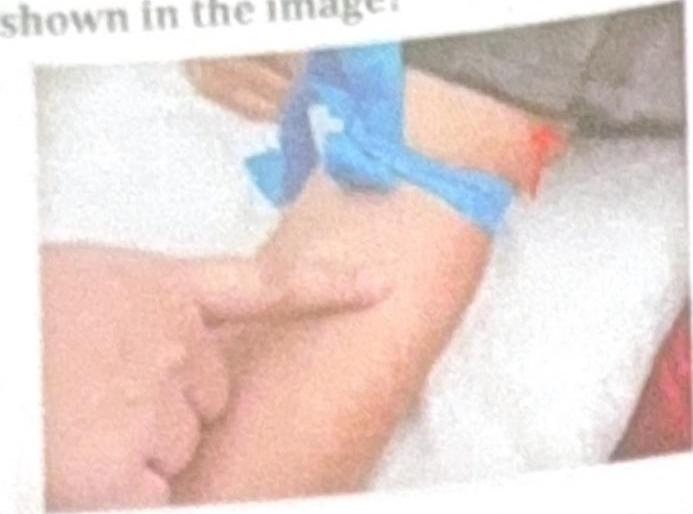
What is the name of the regional anesthetic technique shown in the image?
Which nerve is targeted in the nasociliary nerve block?
The duration of spinal anaesthesia is based directly on:
Spinal anaesthesia in an adult is given at this level:
All are true about management of PDPH except-
What is the concentration of lignocaine used for spinal anesthesia?
First spinal anaesthesia was given by -
Practice by Chapter
Neuraxial Anatomy
Practice Questions
Spinal Anesthesia
Practice Questions
Epidural Anesthesia
Practice Questions
Combined Spinal-Epidural Anesthesia
Practice Questions
Peripheral Nerve Blocks: Upper Extremity
Practice Questions
Peripheral Nerve Blocks: Lower Extremity
Practice Questions
Truncal Blocks
Practice Questions
Ultrasound-Guided Regional Anesthesia
Practice Questions
Complications of Regional Anesthesia
Practice Questions
Regional Anesthesia in Pediatric Patients
Practice Questions
Regional Anesthesia in Obstetrics
Practice Questions
Continuous Peripheral Nerve Catheters
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app