
Regional Anesthesia — MCQs

On this page
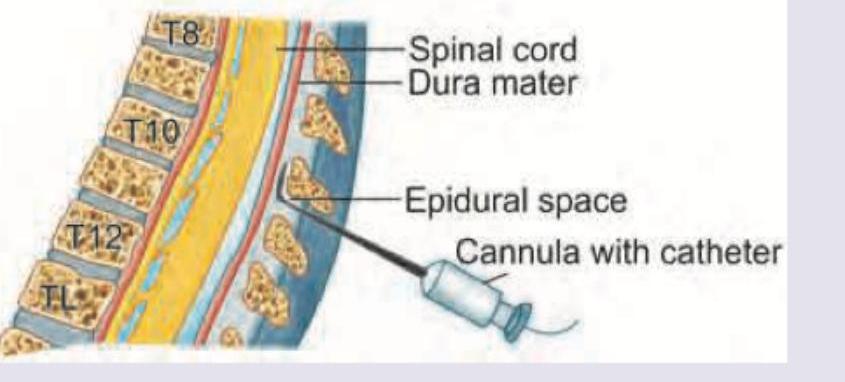
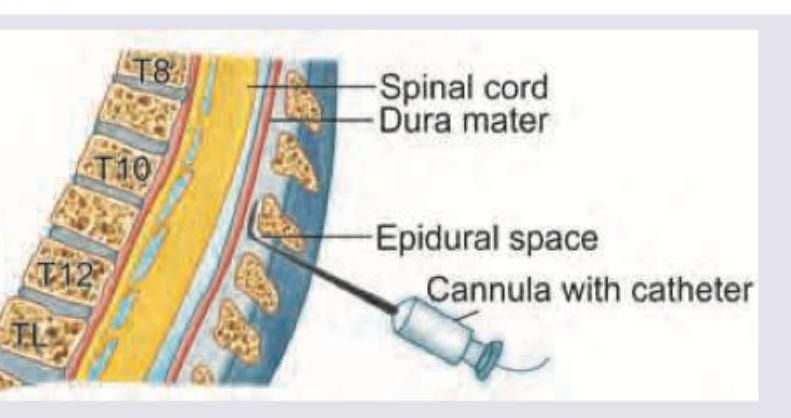
In epidural anesthesia, which of the following layers is least likely to be punctured during the procedure?
Which of the following is most suitable for intravenous regional anesthesia?
During administration of following anesthesia with 10 mL of 2% xylocaine, the patient develops hypotension with respiratory depression. Which of the following is the probable cause? (AIIMS Nov 2016)
All are correct about the regional anesthesia provided to the patient except:

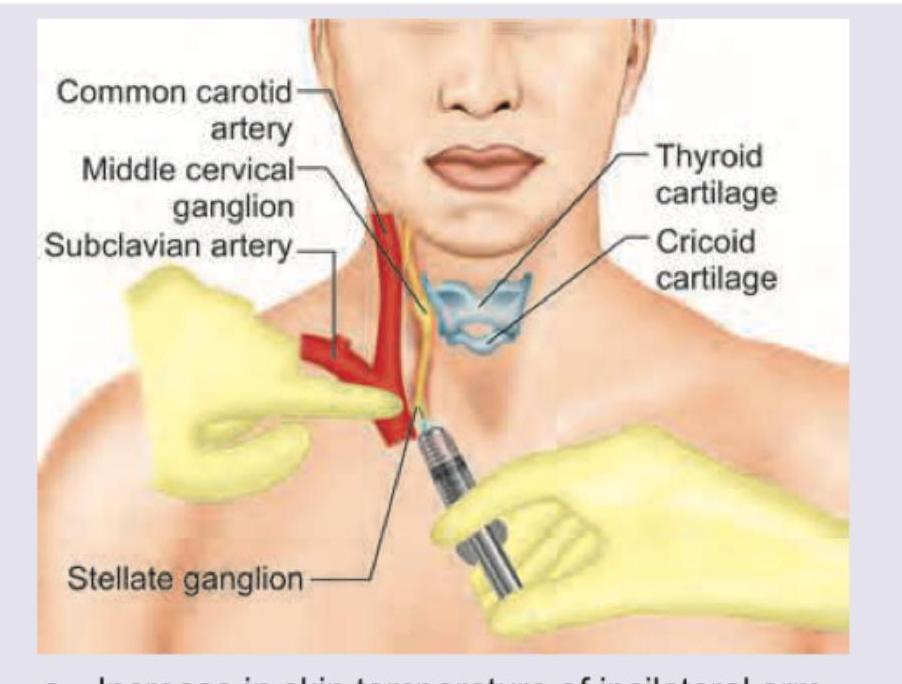
Which is the most reliable objective finding indicating a successful stellate ganglion block? (Recent NEET Pattern 2016-17)
All are correct about the common or classically recognized complications of the anesthesia technique shown except:

All are absolute or relative contraindications of this anesthesia technique except: (Recent NEET Pattern 2016-17)
All of the following are used to prevent or treat post-dural puncture headache except:

All are complications of high spinal anesthesia except: (Recent NEET Pattern 2016-17)

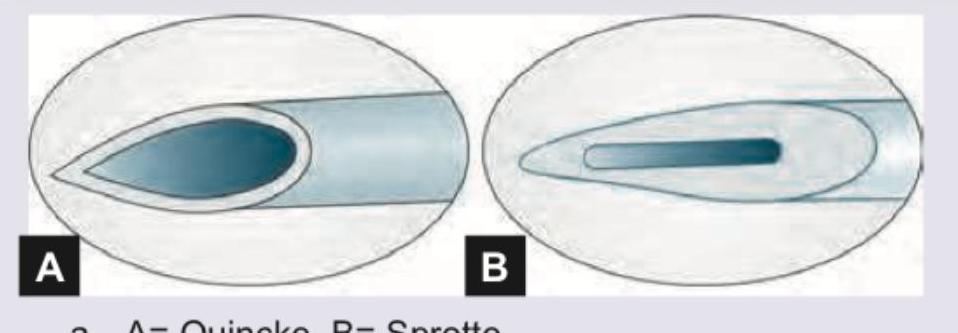
Name the spinal needle shown in the image:
Practice by Chapter
Neuraxial Anatomy
Practice Questions
Spinal Anesthesia
Practice Questions
Epidural Anesthesia
Practice Questions
Combined Spinal-Epidural Anesthesia
Practice Questions
Peripheral Nerve Blocks: Upper Extremity
Practice Questions
Peripheral Nerve Blocks: Lower Extremity
Practice Questions
Truncal Blocks
Practice Questions
Ultrasound-Guided Regional Anesthesia
Practice Questions
Complications of Regional Anesthesia
Practice Questions
Regional Anesthesia in Pediatric Patients
Practice Questions
Regional Anesthesia in Obstetrics
Practice Questions
Continuous Peripheral Nerve Catheters
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app