
Neuroanesthesia — MCQs

On this page
Which of the following drugs does not affect the absorption and secretion of cerebrospinal fluid?
Which of the following increases cerebral oxygen consumption?
Which muscle relaxant is known to increase intracranial pressure?
If pneumocephalus is created either by surgery or by performance of a pneumoencephalogram, it is suggested that nitrous oxide be avoided for how many days?
Which inhalational agent is used in patients with raised intracranial tension?
A patient is scheduled for neurosurgery for posterior fossa tumor. During the surgery the BP crashes and Et CO2 suddenly decreases to zero. All are true regarding the condition leading to this catastrophe except:
A patient is scheduled for neurosurgery for posterior fossa tumor. During the surgery the BP crashes and Et CO2 suddenly decreases to zero. What is the most likely diagnosis?
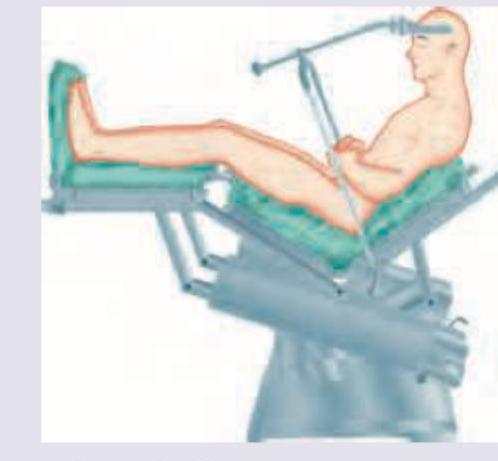
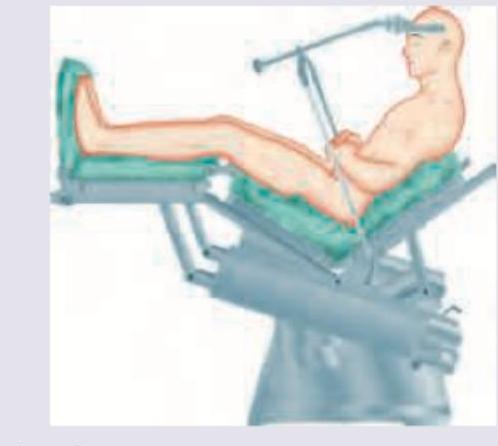
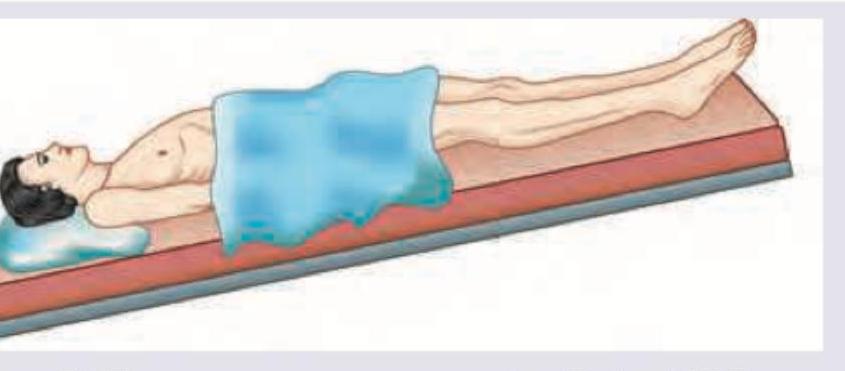
The position of the patient as shown below is favored for which of the following conditions?
Anesthetic agent contraindicated in raised ICT is?
All of the following lower intracranial pressure except?
Practice by Chapter
Cerebral Physiology and Pathophysiology
Practice Questions
Anesthetics and Cerebral Blood Flow
Practice Questions
Intracranial Pressure Management
Practice Questions
Anesthesia for Supratentorial Craniotomy
Practice Questions
Anesthesia for Infratentorial Craniotomy
Practice Questions
Anesthesia for Traumatic Brain Injury
Practice Questions
Neuromonitoring Techniques
Practice Questions
Anesthesia for Spine Surgery
Practice Questions
Anesthesia for Neurovascular Procedures
Practice Questions
Awake Craniotomy
Practice Questions
Neuromuscular Disorders
Practice Questions
Postoperative Care in Neurosurgical Patients
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app