
Thorax — MCQs

On this page
What is the arterial supply of the trachea?
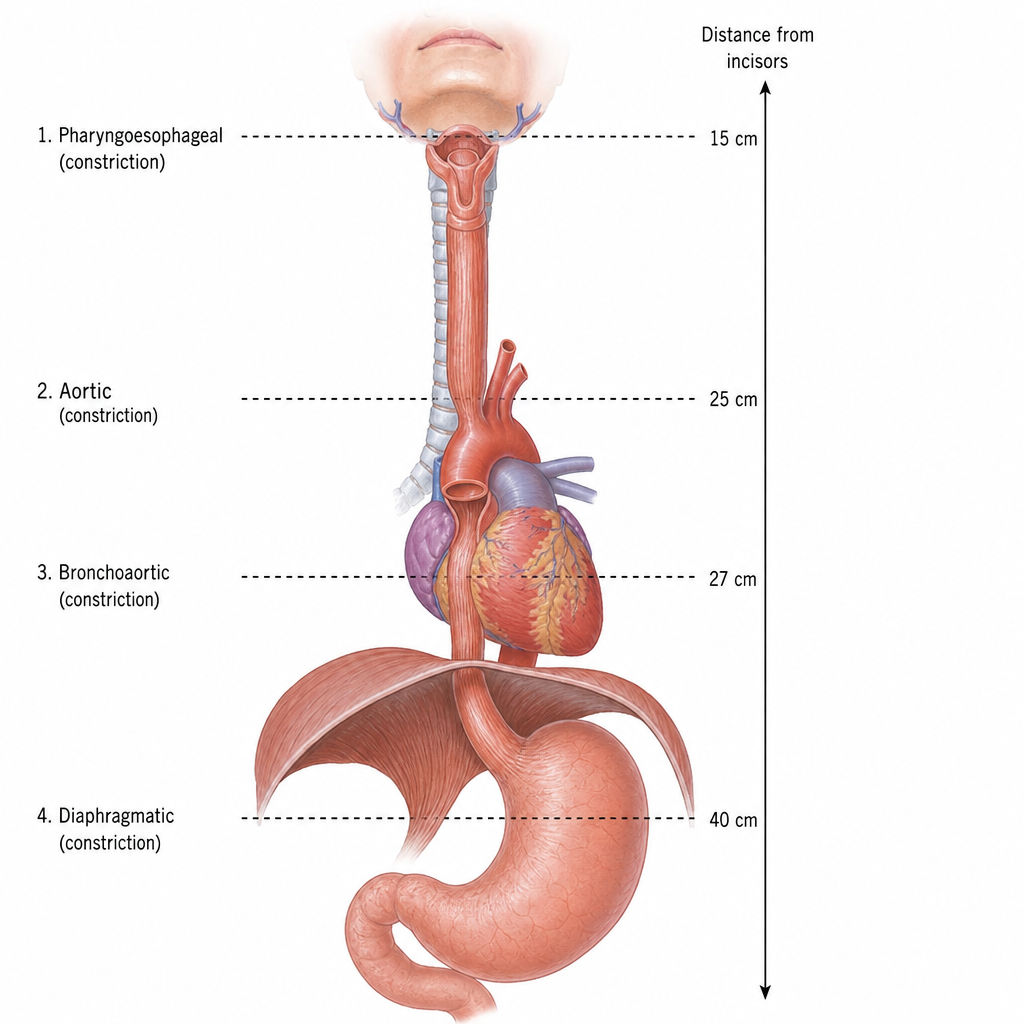
What is the distance of the aortic esophageal constriction from the upper incisors?
Which statement best describes the anatomical difference between the right and left main bronchus?
All of the following are direct articulations of the true rib except?
The anterosuperior surface of the heart is primarily formed by which chamber?
What are the blood vessels supplying the lungs?
Which of the following statements about the venous drainage of the heart is incorrect?
What anatomical structure lies anterior to the transverse sinus?
A 39-year-old man presents with odynophagia. Imaging reveals an esophageal constriction at the level of the diaphragm, and biopsy confirms esophageal cancer. Which of the following lymph nodes will most likely be affected first?
What is the approximate length of the esophagus in an adult?
Practice by Chapter
Thoracic Wall and Diaphragm
Practice Questions
Pleura and Lungs
Practice Questions
Mediastinum
Practice Questions
Heart and Pericardium
Practice Questions
Great Vessels and Azygos System
Practice Questions
Thoracic Duct and Lymphatics
Practice Questions
Autonomic Innervation
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Thoracic Imaging and Cross-sectional Anatomy
Practice Questions
Embryological Development of Thoracic Structures
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app